From the MRC Centre for Neuromuscular Diseases (J.M.M., M.R.B.E., C.D.J.S., T.A.Y., M.G.H., J.S.T., M.M.R.) and Neuroradiological Academic Unit (S.S.), UCL Institute of Neurology, London, UK; Carver College of Medicine (T.G., P.N., M.E.S.) and Department of Radiology (D.T.), University of Iowa, Iowa City.
Neurology. 2018 Sep 18;91(12):e1125-e1129. doi: 10.1212/WNL.0000000000006214. Epub 2018 Aug 17.
To translate the quantitative MRC Centre MRI protocol in Charcot-Marie-Tooth disease type 1A (CMT1A) to a second site; validate its responsiveness in an independent cohort; and test the benefit of participant stratification to increase outcome measure responsiveness.
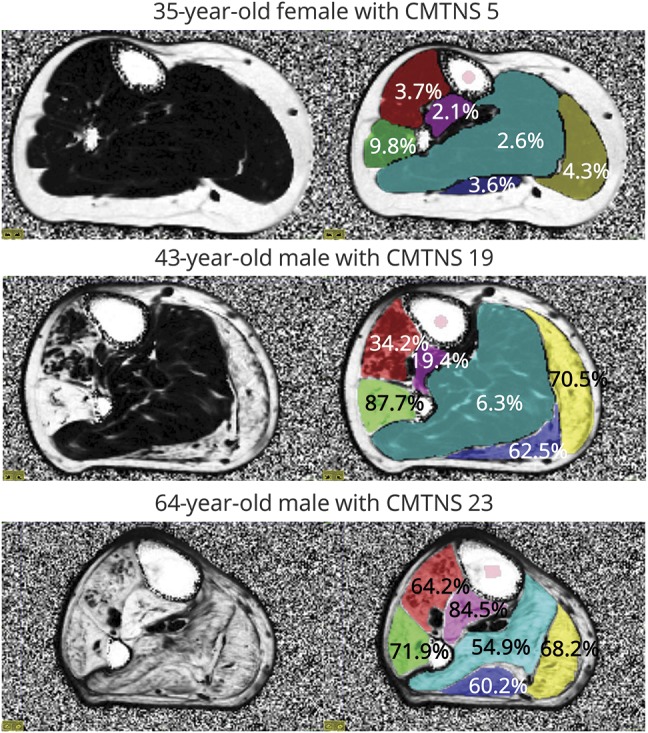
Three healthy volunteers were scanned for intersite standardization. For the longitudinal patient study, 11 patients with CMT1A were recruited with 10 patients rescanned at a 12-month interval. Three-point Dixon MRI of leg muscles was performed to generate fat fraction (FF) maps, transferred to a central site for quality control and analysis. Clinical data collected included CMT Neuropathy Score.
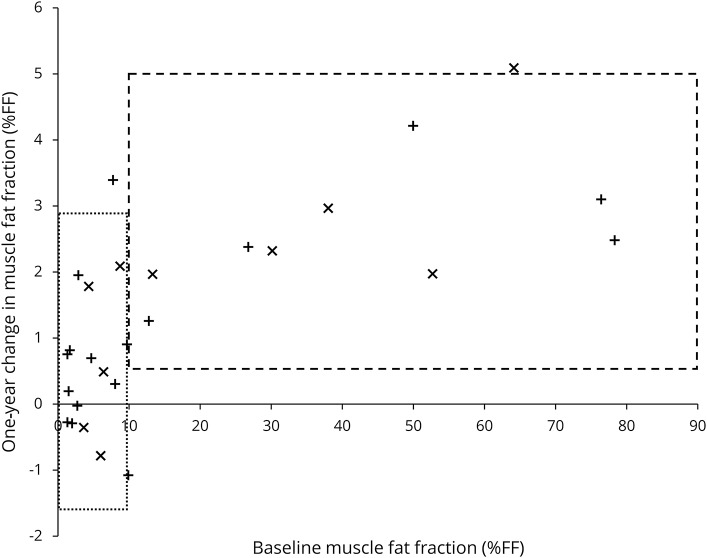
Test-retest reliability of FF within individual healthy calf muscles at the remote site was excellent: intraclass correlation coefficient 0.79, limits of agreement -0.67 to +0.85 %FF. In patients, mean calf muscle FF was 21.0% and correlated strongly with disease severity and age. Calf muscle FF significantly increased over 12 months (+1.8 ± 1.7 %FF, = 0.009). Patients with baseline FF >10% showed a 12-month FF increase of 2.9% ± 1.3% (standardized response mean = 2.19).
We have validated calf muscle FF as an outcome measure in an independent cohort of patients with CMT1A. Responsiveness is significantly improved by enrolling a stratified patient cohort with baseline calf FF >10%.
将定量 MRC 中心肌病磁共振成像(CMT1A)协议转化为第二站点;在独立队列中验证其反应能力;并测试参与者分层的益处,以提高结果测量的反应能力。
对 3 名健康志愿者进行扫描以进行站点间标准化。对于纵向患者研究,招募了 11 名 CMT1A 患者,其中 10 名患者在 12 个月的间隔时间内重新扫描。对腿部肌肉进行三点 Dixon MRI 以生成脂肪分数(FF)图,并将其传输到中心站点进行质量控制和分析。收集的临床数据包括 CMT 神经病评分。
在远程站点,个体健康小腿肌肉内的 FF 测试-再测试可靠性非常好:组内相关系数为 0.79,一致性界限为-0.67 至+0.85 %FF。在患者中,平均小腿肌肉 FF 为 21.0%,与疾病严重程度和年龄密切相关。小腿肌肉 FF 在 12 个月内显著增加(+1.8 ± 1.7 %FF,= 0.009)。基线 FF >10%的患者在 12 个月时的 FF 增加了 2.9%±1.3%(标准化反应均值=2.19)。
我们已经在独立的 CMT1A 患者队列中验证了小腿肌肉 FF 作为一种结果测量方法。通过招募基线小腿 FF >10%的分层患者队列,反应能力显著提高。