Fourrier Célia, Sampson Emma, Mills Natalie T, Baune Bernhard T
Discipline of Psychiatry, University of Adelaide, Adelaide, Australia.
Department of Psychiatry, Melbourne Medical School, The University of Melbourne, Parkville, 3010, VIC, Australia.
Trials. 2018 Aug 20;19(1):447. doi: 10.1186/s13063-018-2829-7.
In patients with major depressive disorder (MDD), antidepressant response and remission rates are low, highlighting the need for new treatment approaches. Recently, the abundant literature linking inflammatory processes and depressive symptoms have led to the hypothesis that selecting treatment for MDD based on the patient's inflammatory status could be a promising strategy to improve outcomes in patients suffering from MDD. The aim of the randomised control trial we propose is to investigate the antidepressant efficacy of the combined treatment of MDD with antidepressant medication plus anti-inflammatory medication in individuals with raised inflammation levels. For the first time, this study will prospectively test the efficacy of an antidepressant plus anti-inflammatory augmentation based on baseline inflammatory maker levels in MDD using a randomised controlled trial design.
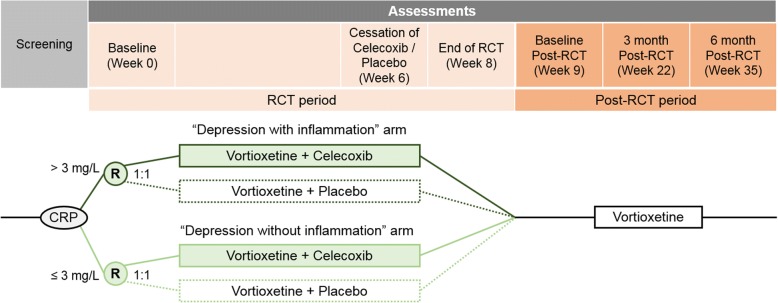
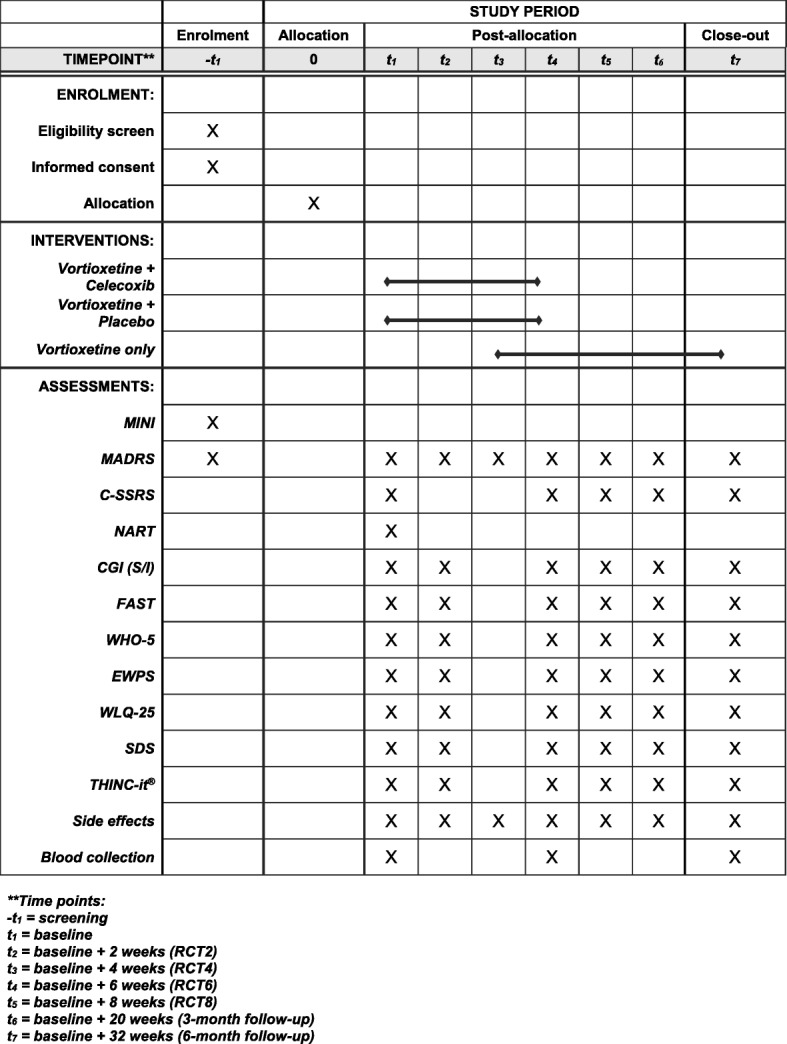
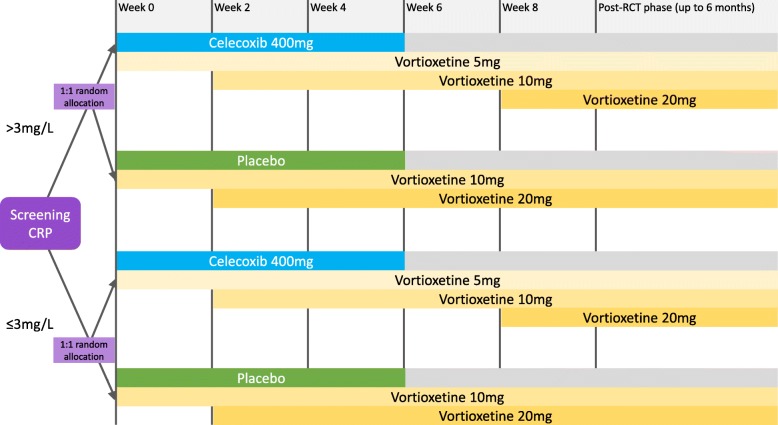
This study proposes to measure blood C-reactive protein (CRP) levels before the initiation of treatment in 200 participants with MDD. Study participants are then assigned into one of two study strata: either into the 'Depression with inflammation' stratum (CRP levels > 3 mg/L); or into the 'Depression without inflammation' stratum (CRP levels ≤ 3 mg/L). Within each of the two study strata, participants randomly receive either antidepressant medication alone (vortioxetine) plus anti-inflammatory medication (celecoxib) or vortioxetine plus placebo for six weeks. At the end of the treatment period, participants have the opportunity to continue vortioxetine alone for a six-month post-trial period. Clinical outcomes are measured at baseline, fortnightly during the treatment period and at the three-month and six-month post-trial visits. The primary outcome is change in MADRS score, with a primary endpoint of a score reduction by 50% from baseline to six weeks (end of augmentation treatment with celecoxib). Secondary clinical outcomes are changes in the cognitive dimensions of depression (cognitive function, emotion processing and social cognition). Biological outcome measures (levels of CRP and other inflammatory markers) are measured at baseline, after six weeks of treatment and at the six-month post-trial visit.
The current study will generate novel evidence for biomarker-based personalised antidepressant treatment selection based on patient inflammatory status before treatment.
Australian New Zealand Clinical Trials Registry (ANZCTR), ACTRN12617000527369p . Registered on 11 April 2017.
在重度抑郁症(MDD)患者中,抗抑郁药的反应率和缓解率较低,这凸显了对新治疗方法的需求。最近,大量将炎症过程与抑郁症状联系起来的文献提出了这样一种假设,即根据患者的炎症状态为MDD选择治疗方法可能是改善MDD患者治疗效果的一种有前景的策略。我们提议进行的随机对照试验的目的是研究在炎症水平升高的个体中,抗抑郁药物联合抗炎药物治疗MDD的抗抑郁疗效。本研究将首次使用随机对照试验设计,基于MDD患者的基线炎症标志物水平,前瞻性地测试抗抑郁药加抗炎药增效治疗的疗效。
本研究提议在200名MDD患者开始治疗前测量其血液C反应蛋白(CRP)水平。然后将研究参与者分为两个研究层之一:要么进入“伴有炎症的抑郁症”层(CRP水平>3mg/L);要么进入“不伴有炎症的抑郁症”层(CRP水平≤3mg/L)。在这两个研究层中,参与者随机接受单独的抗抑郁药物(伏硫西汀)加抗炎药物(塞来昔布)或伏硫西汀加安慰剂治疗六周。在治疗期结束时,参与者有机会在试验后六个月内继续单独服用伏硫西汀。在基线、治疗期间每两周以及试验后三个月和六个月的随访中测量临床结果。主要结局是蒙哥马利-艾森伯格抑郁量表(MADRS)评分的变化,主要终点是从基线到六周(塞来昔布增效治疗结束时)评分降低50%。次要临床结局是抑郁的认知维度(认知功能、情绪加工和社会认知)的变化。在基线、治疗六周后以及试验后六个月的随访中测量生物学结局指标(CRP和其他炎症标志物的水平)。
当前研究将为基于治疗前患者炎症状态的生物标志物个性化抗抑郁治疗选择产生新的证据。
澳大利亚新西兰临床试验注册中心(ANZCTR),ACTRN12617000527369p。于2017年4月11日注册。