Colice Gene, Chisholm Alison, Dima Alexandra L, Reddel Helen K, Burden Annie, Martin Richard J, Brusselle Guy, Popov Todor A, von Ziegenweidt Julie, Price David B
Global Medicines Development, AstraZeneca, Gaithersburg, MD, USA.
Respiratory Effectiveness Group, Cambridge, UK.
Pragmat Obs Res. 2018 Aug 10;9:29-42. doi: 10.2147/POR.S151615. eCollection 2018.
Observational research is essential to evaluate the real-life effectiveness of asthma treatments and can now make use of outcomes derived from electronic medical records.
The aim of this study was to investigate the utility of several database outcome measures in asthma.
This study identified cohorts of patients with active asthma from a UK primary care database - Optimum Patient Care Research Database - approximately 10% of which was prospectively supplemented with questionnaire data. The "Questionnaire cohort" included patients aged 18-60 years with valid questionnaire data and 1 year of continuous primary care data. Separate "ICS initiation" and "ICS step-up" cohorts included patients aged 5-60 years initiated on inhaled corticosteroids (ICSs), who had 1 year of continuous primary care data before, and after, this index visit. Database measures of asthma symptom control and exacerbations were identified in the Optimum Patient Care Research Database and cross-tabulated with corresponding patient-reported (questionnaire) data. Responsiveness of the database outcomes was analyzed, using McNemar's and Wilcoxon's signed rank tests, and Poisson regression was used to estimate the association between database outcomes and future risk of database exacerbations, in the ICS initiation cohort.
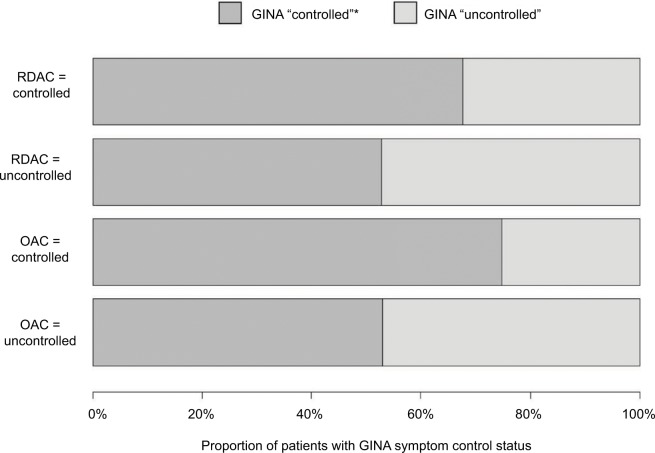
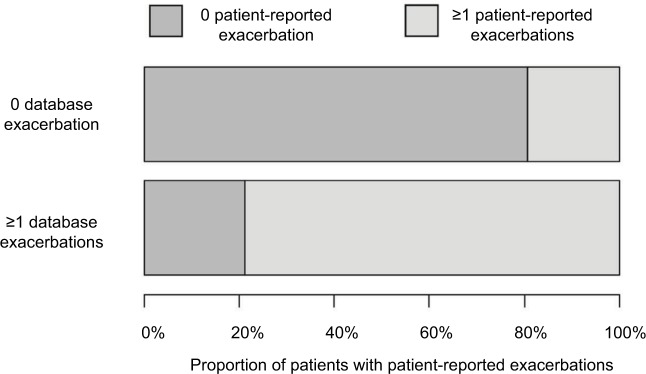
The final study included 2,366 Questionnaire cohort patients and 51,404 ICS initiation patients. Agreement between patient-reported and database-recorded exacerbations was fair (kappa 0.35). Following the initiation of ICS, database risk domain asthma control (based on exacerbations) improved (proportion of patients with uncontrolled asthma decreased from 24.9% to 18.6%; <0.001) and mean number of database exacerbations decreased from 0.09 to 0.08 per patient per year (=0.001). However, another measure of asthma control which includes short-acting beta-agonist prescription as part of the definition did not show this improvement. Patients with prior exacerbations had a higher risk of future exacerbation (rate ratio [95% confidence interval], 3.23 [3.03-3.57]).
Asthma control and exacerbations derived from primary care databases were responsive, with the exception of short-acting beta-agonist prescriptions, and useful for risk prediction.
观察性研究对于评估哮喘治疗的实际疗效至关重要,并且现在可以利用电子病历得出的结果。
本研究的目的是调查几种数据库结局指标在哮喘中的效用。
本研究从英国初级医疗数据库——最佳患者护理研究数据库中确定了活动性哮喘患者队列,其中约10%前瞻性地补充了问卷数据。“问卷队列”包括年龄在18至60岁之间、有有效问卷数据且有1年连续初级医疗数据的患者。单独的“ICS起始”和“ICS升级”队列包括年龄在5至60岁之间开始使用吸入性糖皮质激素(ICS)的患者,这些患者在本次索引就诊之前和之后有1年连续的初级医疗数据。在最佳患者护理研究数据库中确定哮喘症状控制和加重的数据库指标,并与相应的患者报告(问卷)数据进行交叉制表。使用McNemar检验和Wilcoxon符号秩检验分析数据库结局的反应性,并使用泊松回归估计ICS起始队列中数据库结局与未来数据库加重风险之间的关联。
最终研究纳入了2366名问卷队列患者和51404名ICS起始患者。患者报告的加重与数据库记录的加重之间的一致性一般(kappa值为0.35)。开始使用ICS后,数据库风险领域的哮喘控制(基于加重情况)有所改善(未控制哮喘的患者比例从24.9%降至18.6%;P<0.001),每位患者每年的数据库加重平均次数从0.09降至0.08(P=0.001)。然而,另一种将短效β受体激动剂处方作为定义一部分的哮喘控制指标并未显示出这种改善。既往有加重情况的患者未来加重的风险更高(率比[95%置信区间],3.23[3.03 - 3.57])。
除短效β受体激动剂处方外,初级医疗数据库得出的哮喘控制和加重情况指标具有反应性,且对风险预测有用。