Division of Infectious Diseases, Alpert Medical School.
Center for Statistical Sciences, Brown University, Providence, Rhode Island, USA.
AIDS. 2018 Nov 13;32(17):2485-2496. doi: 10.1097/QAD.0000000000001964.
Characterize failure and resistance above and below guidelines-recommended 1000 copies/ml virologic threshold, upon second-line failure.
Cross-sectional study.
Kenyan adults on lopinavir/ritonavir-based second-line were enrolled at AMPATH (Academic Model Providing Access to Healthcare). Charts were reviewed for demographic/clinical characteristics and CD4/viral load were obtained. Participants with detectable viral load had a second visit and pol genotyping was attempted in both visits. Accumulated resistance was defined as mutations in the second, not the first visit. Low-level viremia (LLV) was detectable viral load less than 1000 copies/ml. Failure and resistance associations were evaluated using logistic and Poisson regression, Fisher Exact and t-tests.
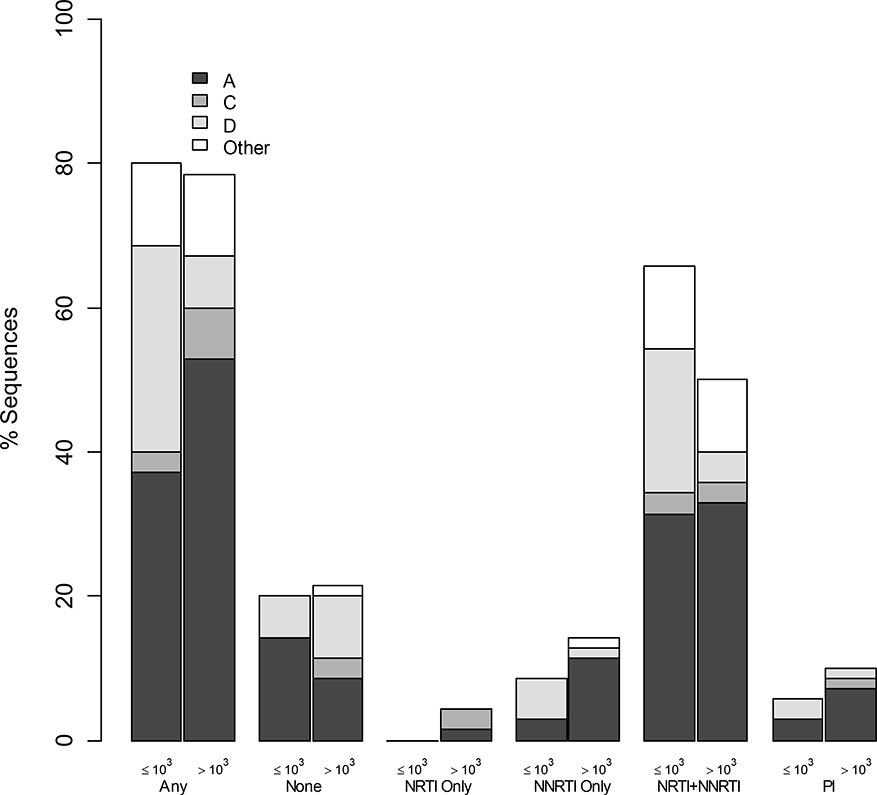
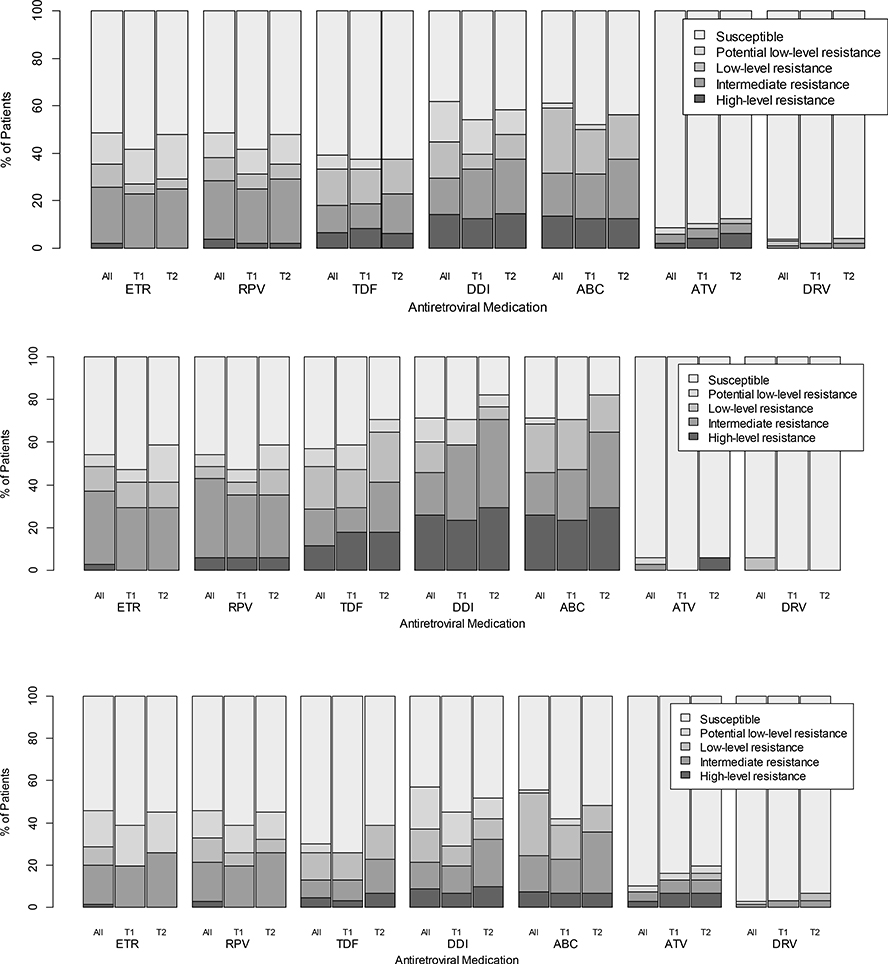
Of 394 participants (median age 42, 60% women, median 1.9 years on second-line) 48% had detectable viral load; 21% had viral load more than 1000 copies/ml, associated with younger age, tuberculosis treatment, shorter time on second-line, lower CD4count/percentage, longer first-line treatment interruption and pregnancy. In 105 sequences from the first visit (35 with LLV), 79% had resistance (57% dual-class, 7% triple-class; 46% with intermediate-to-high-level resistance to ≥1 future drug option). LLV was associated with more overall and NRTI-associated mutations and with predicted resistance to more next-regimen drugs. In 48 second-visit sequences (after median 55 days; IQR 28-33), 40% accumulated resistance and LLV was associated with more mutation accumulation.
High resistance upon second-line failure exists at levels above and below guideline-recommended virologic-failure threshold, impacting future treatment options. Optimization of care should include increased viral load monitoring, resistance testing and third-line ART access, and consideration of lowering the virologic failure threshold, though this demands further investigation.
描述二线治疗失败时,高于和低于指南推荐的 1000 拷贝/ml 病毒学失败阈值的失败和耐药情况。
横断面研究。
在肯尼亚的 AMPATH(提供医疗保健机会的学术模式),入组接受洛匹那韦/利托那韦为基础的二线治疗的成年患者。对图表进行了回顾,以获取人口统计学/临床特征,并获得 CD4/病毒载量。有可检测病毒载量的参与者进行了第二次就诊,并在两次就诊中尝试进行 pol 基因分型。累积耐药定义为第二次就诊而不是第一次就诊时出现的突变。低水平病毒血症(LLV)是指可检测到的病毒载量低于 1000 拷贝/ml。使用逻辑回归和泊松回归、Fisher 精确检验和 t 检验评估失败和耐药相关性。
在 394 名参与者中(中位年龄 42 岁,60%为女性,二线治疗中位时间 1.9 年),48%有可检测到的病毒载量;21%的病毒载量超过 1000 拷贝/ml,与年龄较小、结核病治疗、二线治疗时间较短、CD4 计数/百分比较低、一线治疗中断时间较长和妊娠有关。在第一次就诊的 105 个序列中(35 个为 LLV),79%有耐药性(57%双重耐药,7%三重耐药;46%对至少一种未来药物选择具有中高水平耐药性)。LLV 与更多的总耐药和 NRTI 相关突变以及更多未来方案药物的预测耐药性有关。在 48 个第二次就诊的序列中(中位时间为 55 天后,IQR 28-33),40%累积耐药,LLV 与更多突变积累有关。
二线治疗失败时,存在高于和低于指南推荐的病毒学失败阈值的高耐药性,这影响了未来的治疗选择。应优化护理,包括增加病毒载量监测、耐药性检测和三线 ART 治疗,考虑降低病毒学失败阈值,尽管这需要进一步研究。