Yotsu Rie R, Richardson Marty, Ishii Norihisa
Department of Dermatology, National Center for Global Health and Medicine, 1-21-1 Toyama, Shinjuku-ku, Tokyo, Japan, 162-8655.
Cochrane Database Syst Rev. 2018 Aug 23;8(8):CD012118. doi: 10.1002/14651858.CD012118.pub2.
Buruli ulcer is a necrotizing cutaneous infection caused by infection with Mycobacterium ulcerans bacteria that occurs mainly in tropical and subtropical regions. The infection progresses from nodules under the skin to deep ulcers, often on the upper and lower limbs or on the face. If left undiagnosed and untreated, it can lead to lifelong disfigurement and disabilities. It is often treated with drugs and surgery.
To summarize the evidence of drug treatments for treating Buruli ulcer.
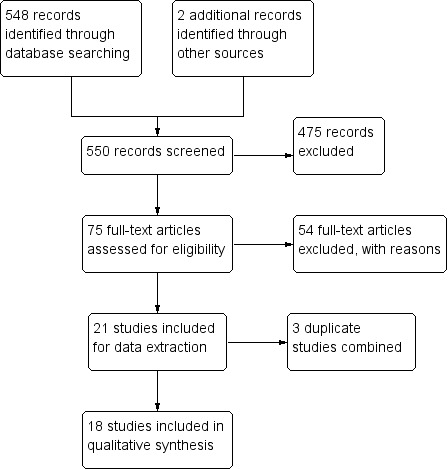
We searched the Cochrane Infectious Diseases Group Specialized Register; the Cochrane Central Register of Controlled Trials (CENTRAL), published in the Cochrane Library; MEDLINE (PubMed); Embase (Ovid); and LILACS (Latin American and Caribbean Health Sciences Literature; BIREME). We also searched the US National Institutes of Health Ongoing Trials Register (clinicaltrials.gov) and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/search/en/). All searches were run up to 19 December 2017. We also checked the reference lists of articles identified by the literature search, and contacted leading researchers in this topic area to identify any unpublished data.
We included randomized controlled trials (RCTs) that compared antibiotic therapy to placebo or alternative therapy such as surgery, or that compared different antibiotic regimens. We also included prospective observational studies that evaluated different antibiotic regimens with or without surgery.
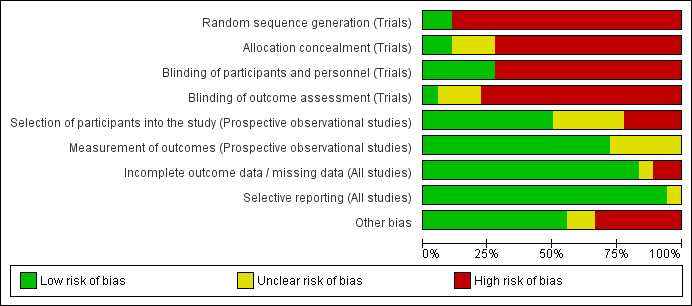
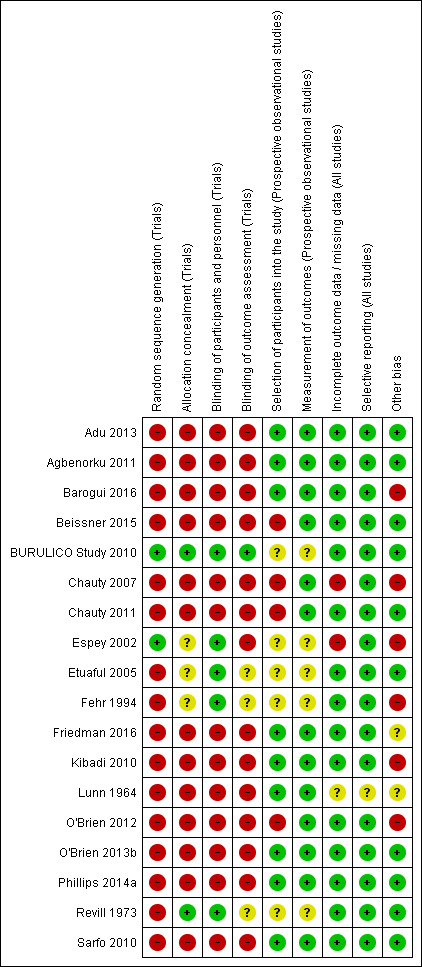
Two review authors independently applied the inclusion criteria, extracted the data, and assessed methodological quality. We calculated the risk ratio (RR) for dichotomous data with 95% confidence intervals (CI). We assessed the certainty of the evidence using the GRADE approach.
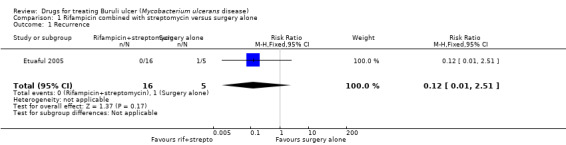
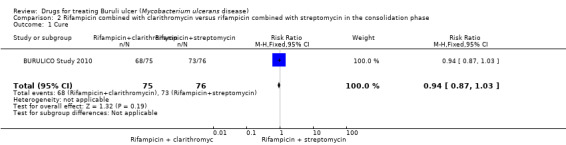
We included a total of 18 studies: five RCTs involving a total of 319 participants, ranging from 12 participants to 151 participants, and 13 prospective observational studies, with 1665 participants. Studies evaluated various drugs usually in addition to surgery, and were carried out across eight countries in areas with high Buruli ulcer endemicity in West Africa and Australia. Only one RCT reported adequate methods to minimize bias. Regarding monotherapy, one RCT and one observational study evaluated clofazimine, and one RCT evaluated sulfamethoxazole/trimethoprim. All three studies had small sample sizes, and no treatment effect was demonstrated. The remaining studies examined combination therapy.Rifampicin combined with streptomycinWe found one RCT and six observational studies which evaluated rifampicin combined with streptomycin for different lengths of treatment (2, 4, 8, or 12 weeks) (941 participants). The RCT did not demonstrate a difference between the drugs added to surgery compared with surgery alone for recurrence at 12 months, but was underpowered (RR 0.12, 95% CI 0.01 to 2.51; 21 participants; very low-certainty evidence).An additional five single-arm observational studies with 828 participants using this regimen for eight weeks with surgery (given to either all participants or to a select group) reported healing rates ranging from 84.5% to 100%, assessed between six weeks and one year. Four observational studies reported healing rates for participants who received the regimen alone without surgery, reporting healing rates ranging from 48% to 95% assessed between eight weeks and one year.Rifampicin combined with clarithromycinTwo observational studies administered combined rifampicin and clarithromycin. One study evaluated the regimen alone (no surgery) for eight weeks and reported a healing rate of 50% at 12 months (30 participants). Another study evaluated the regimen administered for various durations (as determined by the clinicians, durations unspecified) with surgery and reported a healing rate of 100% at 12 months (21 participants).Rifampicin with streptomycin initially, changing to rifampicin with clarithromycin in consolidation phaseOne RCT evaluated this regimen (four weeks in each phase) against continuing with rifampicin and streptomycin in the consolidation phase (total eight weeks). All included participants had small lesions, and healing rates were above 90% in both groups without surgery (healing rate at 12 months RR 0.94, 95% CI 0.87 to 1.03; 151 participants; low-certainty evidence). One single-arm observational study evaluating the substitution of streptomycin with clarithromycin in the consolidation phase (6 weeks, total 8 weeks) without surgery given to a select group showed a healing rate of 98% at 12 months (41 participants).Novel combination therapyTwo large prospective studies in Australia evaluated some novel regimens. One study evaluating rifampicin combined with either ciprofloxacin, clarithromycin, or moxifloxacin without surgery reported a healing rate of 76.5% at 12 months (132 participants). Another study evaluating combinations of two to three drugs from rifampicin, ciprofloxacin, clarithromycin, ethambutol, moxifloxacin, or amikacin with surgery reported a healing rate of 100% (90 participants).Adverse effects were reported in only three RCTs (158 participants) and eight prospective observational studies (878 participants), and were consistent with what is already known about the adverse effect profile of these drugs. Paradoxical reactions (clinical deterioration after treatment caused by enhanced immune response to M ulcerans) were evaluated in six prospective observational studies (822 participants), and the incidence of paradoxical reactions ranged from 1.9% to 26%.
AUTHORS' CONCLUSIONS: While the antibiotic combination treatments evaluated appear to be effective, we found insufficient evidence showing that any particular drug is more effective than another. How different sizes, lesions, and stages of the disease may contribute to healing and which kind of lesions are in need of surgery are unclear based on the included studies. Guideline development needs to consider these factors in designing practical treatment regimens. Forthcoming trials using clarithromycin with rifampicin and other trials of new regimens that also address these factors will help to identify the best regimens.
布鲁里溃疡是由溃疡分枝杆菌感染引起的一种坏死性皮肤感染,主要发生在热带和亚热带地区。感染从皮肤下的结节发展为深部溃疡,常见于上肢、下肢或面部。如果不进行诊断和治疗,可能导致终身毁容和残疾。通常采用药物和手术进行治疗。
总结治疗布鲁里溃疡的药物治疗证据。
我们检索了Cochrane传染病组专业注册库;Cochrane图书馆中发表的Cochrane对照试验中心注册库(CENTRAL);医学期刊数据库(MEDLINE,通过PubMed检索);Embase数据库(通过Ovid检索);以及拉丁美洲和加勒比卫生科学文献数据库(LILACS;巴西医学文献数据库,BIREME)。我们还检索了美国国立卫生研究院正在进行的试验注册库(clinicaltrials.gov)和世界卫生组织(WHO)国际临床试验注册平台(ICTRP)(网址:www.who.int/ictrp/search/en/)。所有检索截至2017年12月19日。我们还检查了文献检索所识别文章的参考文献列表,并联系了该主题领域的主要研究人员以识别任何未发表的数据。
我们纳入了比较抗生素疗法与安慰剂或替代疗法(如手术),或比较不同抗生素方案的随机对照试验(RCT)。我们还纳入了评估不同抗生素方案(无论是否联合手术)的前瞻性观察性研究。
两位综述作者独立应用纳入标准,提取数据,并评估方法学质量。我们计算了二分类数据的风险比(RR)及其95%置信区间(CI)。我们使用GRADE方法评估证据的确定性。
我们共纳入了18项研究:5项RCT,共319名参与者,参与者人数从12名到151名不等;以及13项前瞻性观察性研究,共1665名参与者。这些研究通常除手术外还评估了各种药物,研究在西非和澳大利亚布鲁里溃疡高流行地区的8个国家开展。只有1项RCT报告了充分的方法以尽量减少偏倚。关于单一疗法,1项RCT和1项观察性研究评估了氯法齐明,1项RCT评估了磺胺甲恶唑/甲氧苄啶。所有这三项研究样本量均较小,未显示出治疗效果。其余研究考察了联合疗法。
利福平联合链霉素
我们发现1项RCT和6项观察性研究评估了利福平联合链霉素不同疗程(2、4、8或12周)的疗效(941名参与者)。该RCT未显示添加药物的手术组与单纯手术组在12个月复发率上存在差异,但检验效能不足(RR 0.12,95%CI 0.01至2.51;21名参与者;极低确定性证据)。
另外5项单臂观察性研究共828名参与者使用该方案联合手术治疗8周(所有参与者或选定组),报告的愈合率在6周和1年之间评估,范围为84.5%至100%。4项观察性研究报告了未接受手术仅使用该方案的参与者的愈合率,在8周和1年之间评估,愈合率范围为48%至%。
利福平联合克拉霉素
2项观察性研究使用了利福平联合克拉霉素。1项研究单独评估了该方案(未手术)8周,报告12个月时愈合率为50%(30名参与者)。另一项研究评估了该方案联合手术不同疗程(由临床医生确定,疗程未明确),报告12个月时愈合率为100%(21名参与者)。
利福平联合链霉素起始治疗,巩固期换为利福平联合克拉霉素
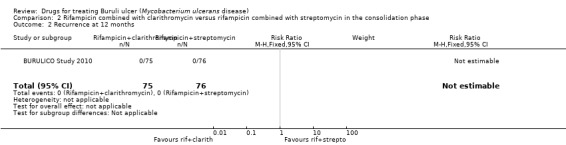
1项RCT评估了该方案(每个阶段4周)与巩固期继续使用利福平联合链霉素(共8周)的疗效对比。所有纳入参与者的皮损均较小,两组在未手术情况下愈合率均高于90%(12个月时愈合率RR 0.94,95%CI 0.87至1.03;151名参与者;低确定性证据)。1项单臂观察性研究评估了选定组在巩固期(6周,共8周)未手术情况下用克拉霉素替代链霉素的疗效,报告12个月时愈合率为98%(41名参与者)。
新型联合疗法
澳大利亚的2项大型前瞻性研究评估了一些新型方案。1项研究评估了利福平联合环丙沙星、克拉霉素或莫西沙星且未手术的方案,报告12个月时愈合率为76.5%(132名参与者)。另一项研究评估了利福平、环丙沙星、克拉霉素、乙胺丁醇、莫西沙星或阿米卡星中两至三种药物联合手术的方案,报告愈合率为100%(90名参与者)。
仅3项RCT(158名参与者)和8项前瞻性观察性研究(878名参与者)报告了不良反应,且与这些药物已知的不良反应特征一致。6项前瞻性观察性研究(822名参与者)评估了矛盾反应(治疗后因对溃疡分枝杆菌免疫反应增强导致的临床病情恶化),矛盾反应发生率范围为1.9%至26%。
虽然所评估的抗生素联合治疗似乎有效,但我们发现证据不足,无法表明任何一种特定药物比另一种更有效。根据纳入的研究,尚不清楚疾病的不同大小、皮损和阶段如何影响愈合,以及哪些类型的皮损需要手术治疗。指南制定在设计实际治疗方案时需要考虑这些因素。即将开展的使用克拉霉素联合利福平的试验以及其他也考虑这些因素的新方案试验将有助于确定最佳方案。