Department of Cardiology, Maastricht University Medical Center, Maastricht, The Netherlands.
Center for Health System Innovation, Keck Medicine of USC, Los Angeles, California, United States of America.
PLoS One. 2020 Jun 30;15(6):e0233457. doi: 10.1371/journal.pone.0233457. eCollection 2020.
Chronic diseases are increasingly prevalent in Western countries. Once hospitalised, the chance for another hospitalisation increases sharply with large impact on well-being of patients and costs. The pattern of readmissions is very complex, but poorly understood for multiple chronic diseases.
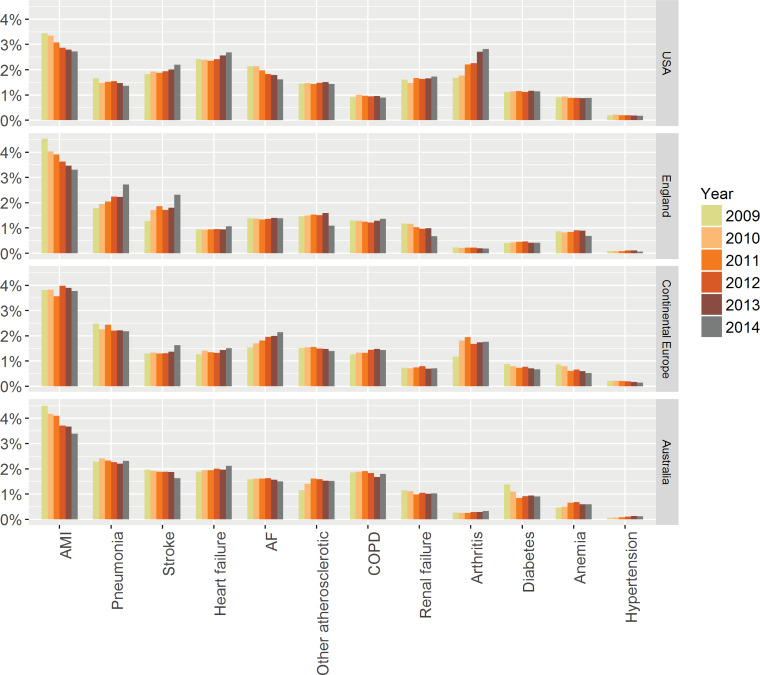
This cohort study of administrative discharge data between 2009-2014 from 21 tertiary hospitals (eight USA, five UK, four Australia, four continental Europe) investigated rates and reasons of readmissions to the same hospital within 30 days after unplanned admission with one of the following chronic conditions; heart failure; atrial fibrillation; myocardial infarction; hypertension; stroke; chronic obstructive pulmonary disease (COPD); bacterial pneumonia; diabetes mellitus; chronic renal disease; anaemia; arthritis and other cardiovascular disease. Proportions of readmissions with similar versus different diseases were analysed.
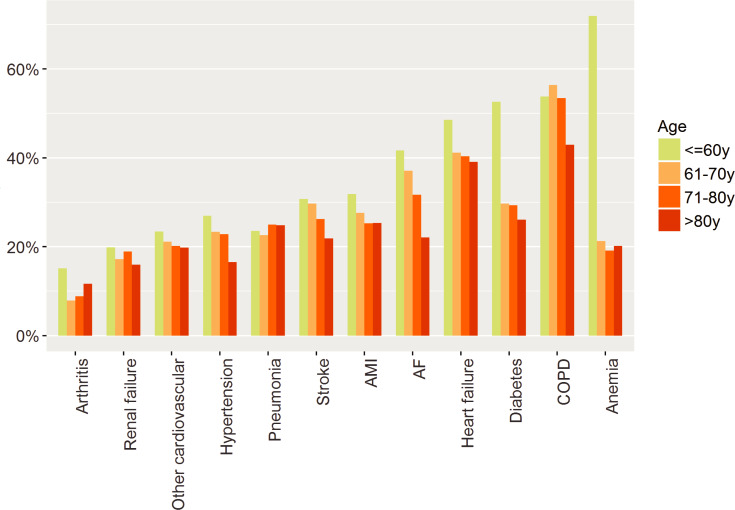
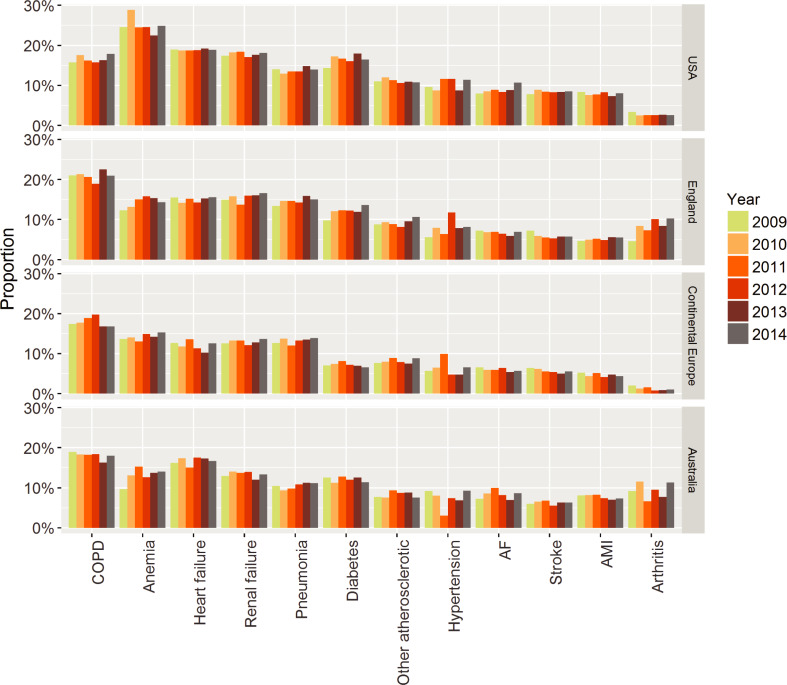
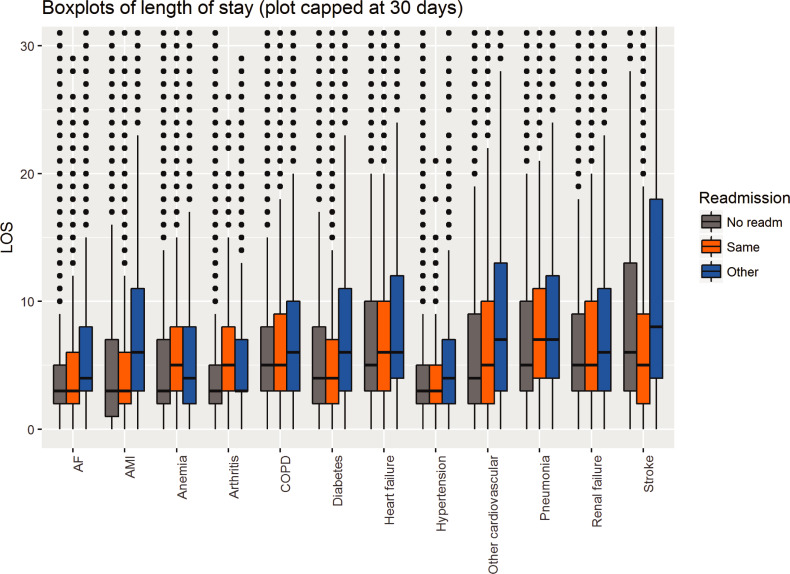
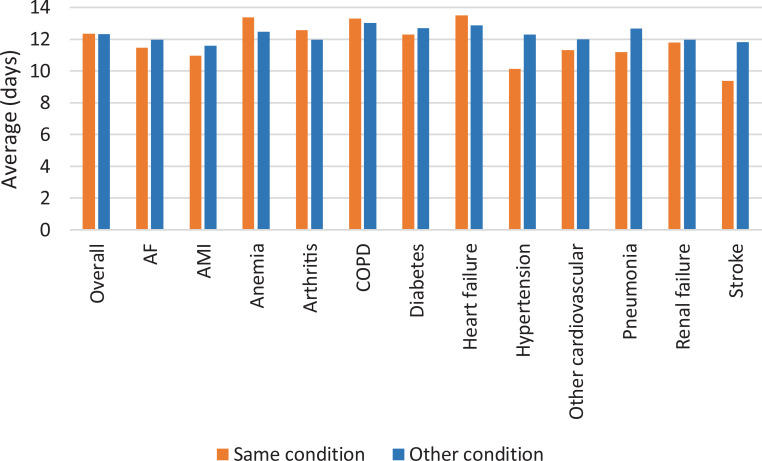
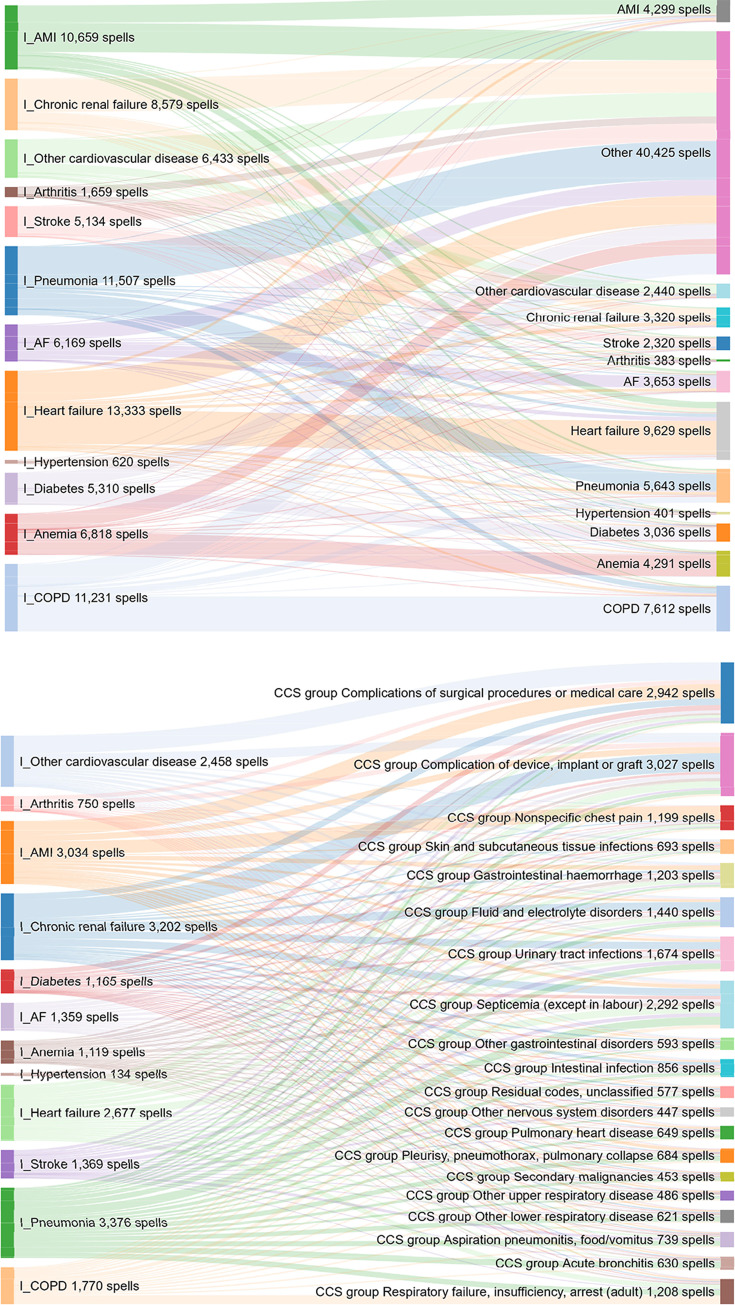
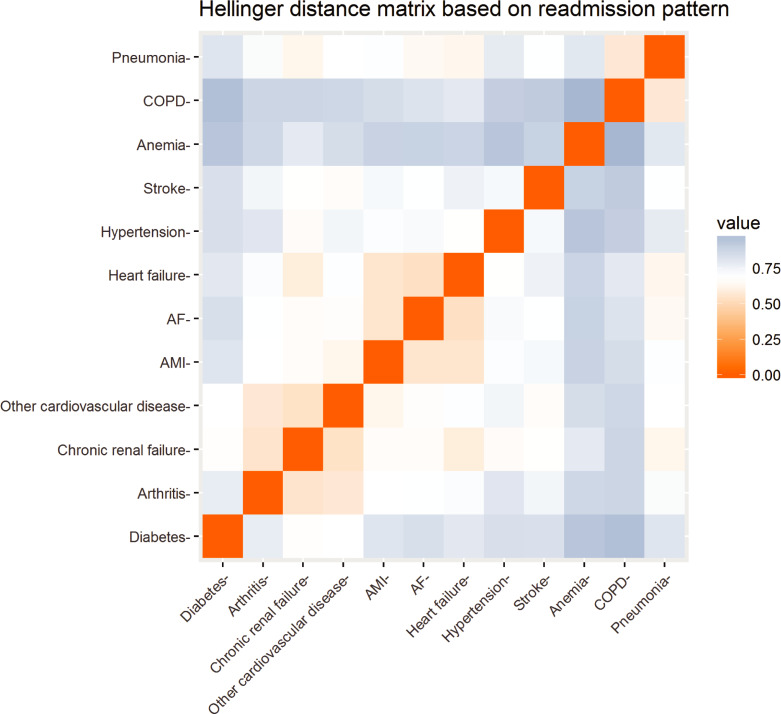
Of 4,901,584 admissions, 866,502 (17.7%) were due to the 12 chronic conditions. In-hospital, 43,573 (5.0%) patients died, leaving 822,929 for readmission analysis. Of those, 87,452 (10.6%) had an emergency 30-day readmission, rates ranged from 2.8% for arthritis to 18.4% for COPD. One third were readmitted with the same condition, ranging from 53% for anaemia to 11% for arthritis. Reasons for readmission were due to another chronic condition in 10% to 35% of the cases, leaving 30% to 70% due to reasons other than the original 12 conditions (most commonly, treatment related complications and infections). The chance of being readmitted with the same cause was lower in the USA, for female patients, with increasing age, more co-morbidities, during study period and with longer initial length of stay.
Readmission in chronic conditions is very common and often caused by diseases other than the index hospitalisation. Interventions to reduce readmissions should therefore focus not only on the primary condition but on a holistic consideration of all the patient's comorbidities.
慢性病在西方国家日益流行。一旦住院,再次住院的机会就会急剧增加,对患者的幸福感和成本都有很大影响。再入院的模式非常复杂,但对于多种慢性病的了解甚少。
这项对 2009 年至 2014 年期间来自 21 家三级医院(美国 8 家、英国 5 家、澳大利亚 4 家、欧洲大陆 4 家)的行政出院数据的队列研究,调查了以下 12 种慢性疾病之一的非计划性入院后 30 天内在同一家医院再次入院的比率和原因:心力衰竭、心房颤动、心肌梗死、高血压、中风、慢性阻塞性肺疾病(COPD)、细菌性肺炎、糖尿病、慢性肾脏病、贫血、关节炎和其他心血管疾病。分析了因相似和不同疾病再次入院的比例。
在 4901584 次入院中,有 866502 次(17.7%)是由 12 种慢性疾病引起的。住院期间,43573 名(5.0%)患者死亡,822929 名患者可用于再入院分析。其中,87452 名(10.6%)有紧急 30 天内再次入院,比率范围从关节炎的 2.8%到 COPD 的 18.4%。三分之一的人因同一疾病再次入院,从贫血的 53%到关节炎的 11%不等。再入院的原因有 10%至 35%是由于另一种慢性疾病,30%至 70%是由于除了最初的 12 种疾病以外的其他原因(最常见的是治疗相关并发症和感染)。在美国,女性患者、年龄较大、合并症较多、研究期间以及初始住院时间较长的患者,再次因同一原因入院的几率较低。
慢性病患者再次入院的情况非常普遍,而且往往是由与住院治疗无关的疾病引起的。因此,减少再入院的干预措施不仅应侧重于主要疾病,还应全面考虑患者的所有合并症。