Division of General Internal Medicine, Weill Cornell Medicine, New York, United States of America.
Center for Global Health, Weill Cornell Medicine, New York, United States of America.
PLoS One. 2018 Aug 29;13(8):e0201945. doi: 10.1371/journal.pone.0201945. eCollection 2018.
Over 18 million adults have initiated life-saving antiretroviral therapy (ART) in resource-poor settings; however, mortality and lost-to-follow-up rates continue to be high among patients in their first year after treatment start. Clinical decision tools are needed to identify patients at high risk for poor outcomes in order to provide individualized risk assessment and intervention. This study aimed to develop and externally validate risk prediction tools that estimate the probability of dying or of being lost to follow-up (LTF) during the year after starting ART.
We used a derivation cohort of 7,031 adults age 15-70 years initiating ART from 2007 to 2013 at 6 clinics in Haiti; 242 (3.5%) had documented death and 1,521 (21.6%) were LTF at 1 year after starting ART. The following routinely collected data were used as predictors in two logistic regression models (one to predict death and another to predict LTF): age, gender, weight, CD4 count, WHO Stage, and diagnosis of tuberculosis (TB). The validation cohort consisted of 1,835 adults initiating ART at a different HIV clinic in Haiti during 2012. We assessed model discrimination by measuring the C-statistic, and measured model calibration by how closely the predicted probabilities approximated actual probabilities of the two outcomes. We derived a nomogram and a point-based risk score from the predictive models.
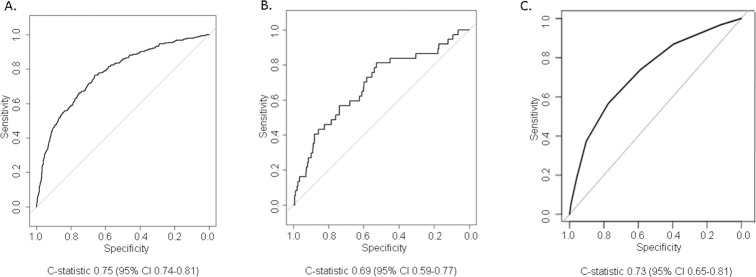
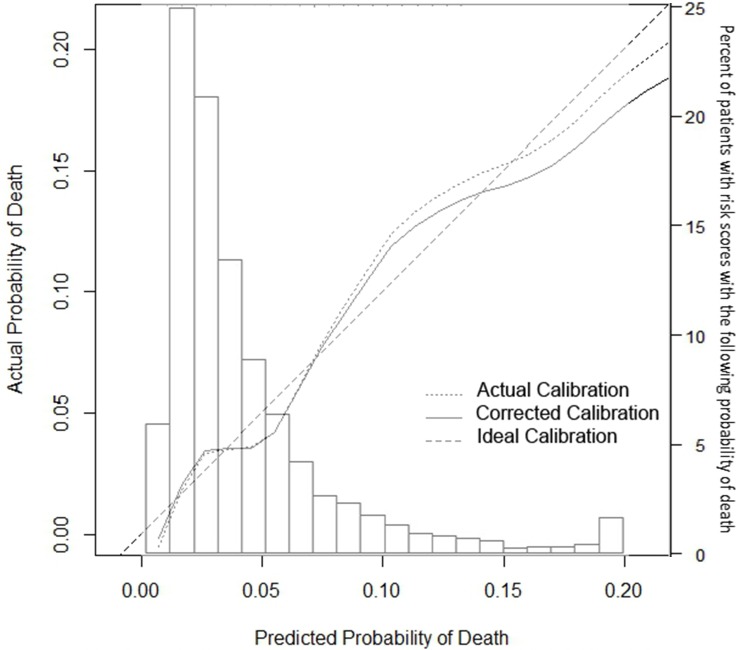
The model predicting death within the year after starting ART had a C-statistic of 0.75 (95% CI 0.74 to 0.81). There was no evidence for significant overfitting and the predictions were well calibrated. The strongest predictors of 1-year mortality were male gender, low weight, low CD4 count, advanced WHO stage, and the absence of TB. In the validation cohort, the C-statistic was 0.69 (95% CI 0.59 to 0.77). A point-based risk score for death had a C-statistic 0.73 (95% CI 0.69 to 0.76) and categorizes patients as low risk (<2% risk of death), average risk (3-4%), and high-risk (8-10%) and very high-risk (14-19%) with likelihood ratios to be used in settings where the baseline risk is different from our study population. The model predicting LTF did not discriminate well (C-statistic 0.59).
A simple risk-score using routinely collected data can predict 1-year mortality after ART initiation for HIV-positive adults in Haiti. However, predicting lost to follow-up using routinely collected data was not as successful. The next step is to assess whether use of this risk score can identify patients who need tailored services to reduce mortality in resource-poor settings such as Haiti.
在资源匮乏的环境中,已有超过 1800 万成年人开始接受救命的抗逆转录病毒疗法(ART);然而,在开始治疗后的第一年,患者的死亡率和失访率仍然很高。需要临床决策工具来识别高风险患者,以便提供个性化的风险评估和干预。本研究旨在开发和外部验证风险预测工具,以估计开始接受 ART 后一年内死亡或失访(LTF)的概率。
我们使用了来自海地 6 个诊所 2007 年至 2013 年期间开始接受 ART 的 7031 名年龄在 15-70 岁的成年人的推导队列;242 人(3.5%)有记录的死亡,1521 人(21.6%)在开始接受 ART 后 1 年时失访。以下是两个逻辑回归模型(一个用于预测死亡,另一个用于预测 LTF)中使用的常规收集数据作为预测因子:年龄、性别、体重、CD4 计数、世界卫生组织(WHO)阶段和结核病(TB)诊断。验证队列由 2012 年在海地另一家 HIV 诊所开始接受 ART 的 1835 名成年人组成。我们通过测量 C 统计量来评估模型的判别能力,通过预测概率与实际两种结果的概率的接近程度来评估模型的校准程度。我们从预测模型中得出了一个诺莫图和一个基于点的风险评分。
预测开始接受 ART 后一年内死亡的模型的 C 统计量为 0.75(95%CI 0.74 至 0.81)。没有证据表明存在显著的过度拟合,并且预测结果校准良好。1 年死亡率的最强预测因素是男性、低体重、低 CD4 计数、晚期 WHO 阶段和无结核病。在验证队列中,C 统计量为 0.69(95%CI 0.59 至 0.77)。基于点的死亡风险评分的 C 统计量为 0.73(95%CI 0.69 至 0.76),并将患者分为低风险(<2%的死亡风险)、平均风险(3-4%)、高风险(8-10%)和极高风险(14-19%),并提供用于在基线风险与我们的研究人群不同的情况下使用的可能性比。预测 LTF 的模型不能很好地区分(C 统计量为 0.59)。
使用常规收集的数据可以预测海地 HIV 阳性成年人开始接受 ART 后 1 年内的死亡率。然而,使用常规收集的数据预测失访率并不成功。下一步是评估使用这种风险评分是否可以识别需要量身定制服务的患者,以降低资源匮乏环境(如海地)的死亡率。