Internal Medicine II, Klinikum rechts der Isar, Technische Universität München, Munich, Germany.
Front Immunol. 2018 Aug 15;9:1878. doi: 10.3389/fimmu.2018.01878. eCollection 2018.
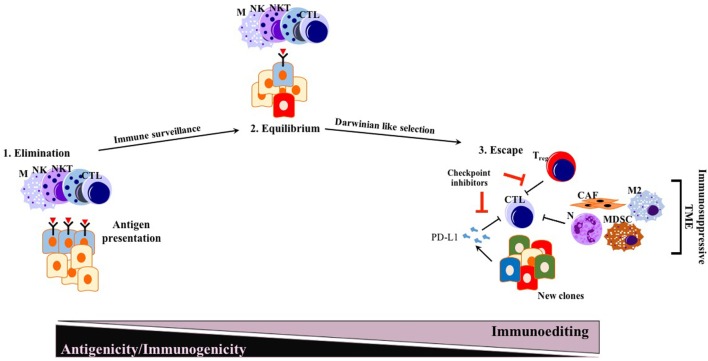
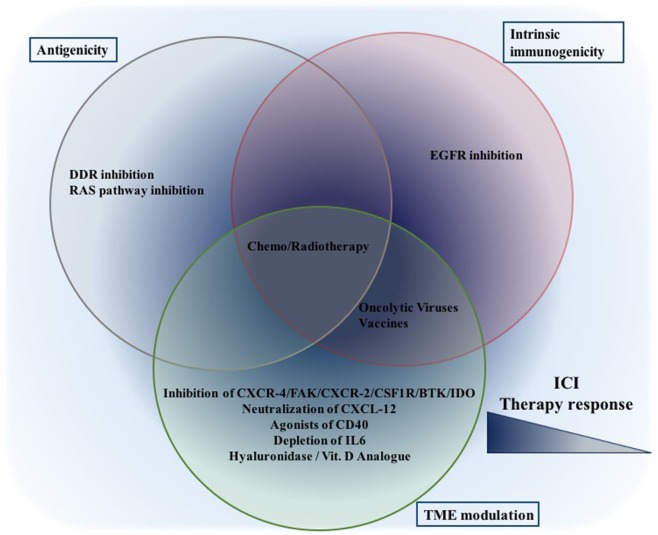
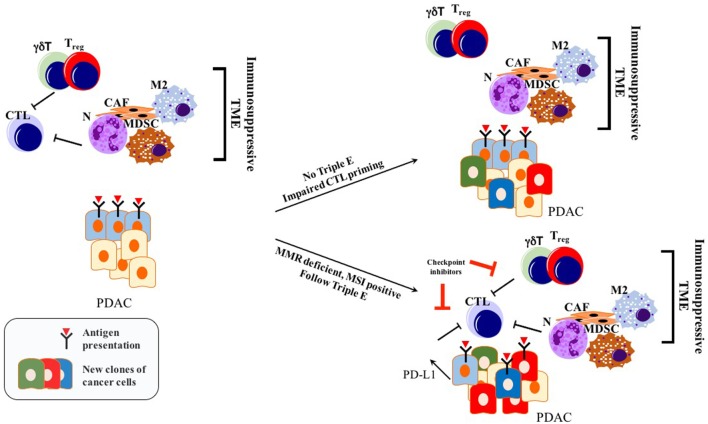
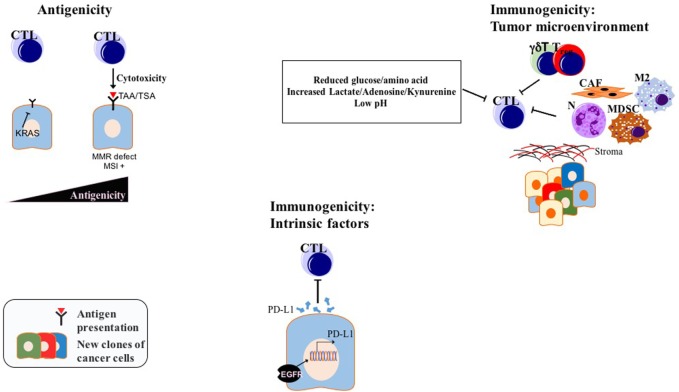
Pancreatic ductal adenocarcinoma (PDAC), as the most frequent form of pancreatic malignancy, still is associated with a dismal prognosis. Due to its late detection, most patients are ineligible for surgery, and chemotherapeutic options are limited. Tumor heterogeneity and a characteristic structure with crosstalk between the cancer/malignant cells and an abundant tumor microenvironment (TME) make PDAC a very challenging puzzle to solve. Thus far, targeted therapies have failed to substantially improve the overall survival of PDAC patients. Immune checkpoint inhibition, as an emerging therapeutic option in cancer treatment, shows promising results in different solid tumor types and hematological malignancies. However, PDAC does not respond well to immune checkpoint inhibitors anti-programmed cell death protein 1 (PD-1) or anti-cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) alone or in combination. PDAC with its immune-privileged nature, starting from the early pre-neoplastic state, appears to escape from the antitumor immune response unlike other neoplastic entities. Different mechanisms how cancer cells achieve immune-privileged status have been hypothesized. Among them are decreased antigenicity and impaired immunogenicity both cancer cell-intrinsic mechanisms and an augmented immunosuppressive TME. Here, we seek to shed light on the recent advances in both bench and bedside investigation of immunotherapeutic options for PDAC. Furthermore, we aim to compile recent data about how PDAC adopts immune escape mechanisms, and how these mechanisms might be exploited therapeutically in combination with immune checkpoint inhibitors, such as PD-1 or CTLA-4 antibodies.
胰腺导管腺癌(PDAC)作为最常见的胰腺恶性肿瘤形式,仍然与预后不良相关。由于其晚期发现,大多数患者不符合手术条件,化疗选择有限。肿瘤异质性和癌细胞与丰富的肿瘤微环境(TME)之间的相互作用的特征结构使 PDAC 成为一个极具挑战性的难题。迄今为止,靶向治疗未能显著改善 PDAC 患者的总生存率。免疫检查点抑制作为癌症治疗中的一种新兴治疗选择,在不同的实体肿瘤类型和血液恶性肿瘤中显示出有希望的结果。然而,PDAC 对免疫检查点抑制剂抗程序性细胞死亡蛋白 1(PD-1)或抗细胞毒性 T 淋巴细胞相关抗原 4(CTLA-4)单独或联合治疗的反应不佳。PDAC 具有免疫特权性质,从早期癌前状态开始,似乎与其他肿瘤实体不同,逃避了抗肿瘤免疫反应。已经假设了癌细胞如何获得免疫特权状态的不同机制。其中包括抗原性降低和免疫原性受损——这两种都是癌细胞内在的机制,以及增强的免疫抑制性 TME。在这里,我们旨在阐明 PDAC 免疫治疗选择的临床前和临床研究的最新进展。此外,我们旨在汇编有关 PDAC 如何采用免疫逃逸机制的最新数据,以及这些机制如何与免疫检查点抑制剂(如 PD-1 或 CTLA-4 抗体)联合治疗以被利用。