Department of Internal Medicine, Mayo Clinic, Jacksonville, FL, USA.
Department of Hematology and Oncology, Mayo Clinic, 4500 San Pablo Road, Jacksonville, FL, 32224, USA.
J Hematol Oncol. 2018 Jan 12;11(1):8. doi: 10.1186/s13045-017-0552-6.
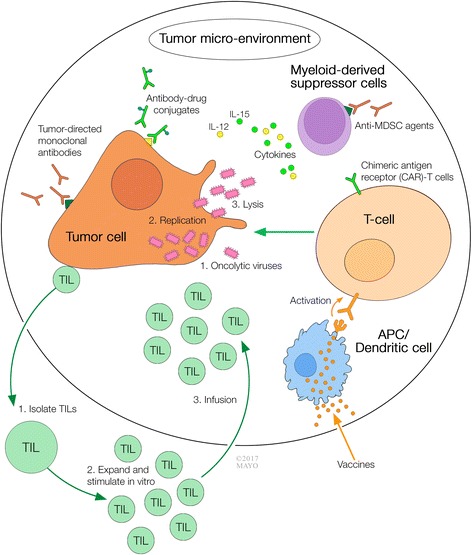
Malignant cells have the capacity to rapidly grow exponentially and spread in part by suppressing, evading, and exploiting the host immune system. Immunotherapy is a form of oncologic treatment directed towards enhancing the host immune system against cancer. In recent years, manipulation of immune checkpoints or pathways has emerged as an important and effective form of immunotherapy. Agents that target cytotoxic T lymphocyte-associated molecule-4 (CTLA-4), programmed cell death receptor-1 (PD-1), and programmed cell death ligand-1 (PD-L1) are the most widely studied and recognized. Immunotherapy, however, extends beyond immune checkpoint therapy by using new molecules such as chimeric monoclonal antibodies and antibody drug conjugates that target malignant cells and promote their destruction. Genetically modified T cells expressing chimeric antigen receptors are able to recognize specific antigens on cancer cells and subsequently activate the immune system. Native or genetically modified viruses with oncolytic activity are of great interest as, besides destroying malignant cells, they can increase anti-tumor activity in response to the release of new antigens and danger signals as a result of infection and tumor cell lysis. Vaccines are also being explored, either in the form of autologous or allogenic tumor peptide antigens, genetically modified dendritic cells that express tumor peptides, or even in the use of RNA, DNA, bacteria, or virus as vectors of specific tumor markers. Most of these agents are yet under development, but they promise to be important options to boost the host immune system to control and eliminate malignancy. In this review, we have provided detailed discussion of different forms of immunotherapy agents other than checkpoint-modifying drugs. The specific focus of this manuscript is to include first-in-human phase I and phase I/II clinical trials intended to allow the identification of those drugs that most likely will continue to develop and possibly join the immunotherapeutic arsenal in a near future.
恶性细胞具有快速指数级生长和扩散的能力,部分原因是它们能够抑制、逃避和利用宿主的免疫系统。免疫疗法是一种针对增强宿主免疫系统对抗癌症的肿瘤治疗方法。近年来,免疫检查点或途径的操纵已成为一种重要且有效的免疫疗法形式。靶向细胞毒性 T 淋巴细胞相关分子 4(CTLA-4)、程序性细胞死亡受体 1(PD-1)和程序性细胞死亡配体 1(PD-L1)的药物是研究最广泛和最受认可的药物。然而,免疫疗法不仅限于免疫检查点疗法,还可以使用新的分子,如嵌合单克隆抗体和抗体药物偶联物,靶向恶性细胞并促进其破坏。表达嵌合抗原受体的基因修饰 T 细胞能够识别癌细胞上的特定抗原,随后激活免疫系统。具有溶瘤活性的天然或基因修饰病毒作为一种非常有吸引力的治疗方法,因为除了破坏恶性细胞外,它们还可以增加抗肿瘤活性,以响应感染和肿瘤细胞裂解导致的新抗原和危险信号的释放。疫苗也在探索中,无论是自体或同种异体肿瘤肽抗原、表达肿瘤肽的基因修饰树突状细胞的形式,甚至使用 RNA、DNA、细菌或病毒作为特定肿瘤标志物的载体。这些药物中的大多数仍处于开发阶段,但它们有望成为增强宿主免疫系统以控制和消除恶性肿瘤的重要选择。在这篇综述中,我们详细讨论了除了检查点修饰药物以外的其他免疫治疗药物。本文的重点是包括首次人体 I 期和 I/II 期临床试验,旨在确定那些最有可能继续开发并在不久的将来可能加入免疫治疗武器库的药物。