Merola Joseph F, Espinoza Luis R, Fleischmann Roy
Department of Dermatology, Medicine and Rheumatology, Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts, USA.
Section of Rheumatology, LSU Health Sciences Center at New Orleans, New Orleans, Louisiana, USA.
RMD Open. 2018 Aug 13;4(2):e000656. doi: 10.1136/rmdopen-2018-000656. eCollection 2018.
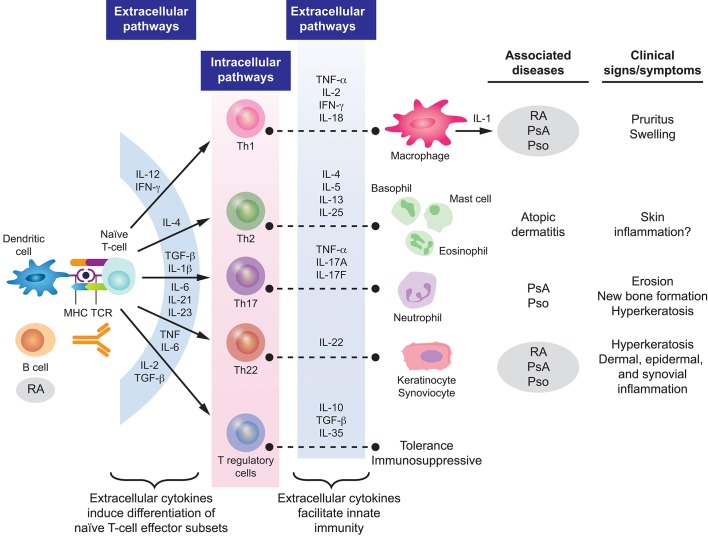
Rheumatoid arthritis (RA) and psoriatic arthritis (PsA) have key differences in clinical presentation, radiographic findings, comorbidities and pathogenesis to distinguish between these common forms of chronic inflammatory arthritis. Joint involvement is typically, but not always, asymmetric in PsA, while it is predominantly symmetric in RA. Bone erosions, without new bone growth, and cervical spine involvement are distinctive of RA, while axial spine involvement, psoriasis and nail dystrophy are distinctive of PsA. Patients with PsA typically have seronegative test findings for rheumatoid factor (RF) and cyclic citrullinated peptide (CCP) antibodies, while approximately 80% of patients with RA have positive findings for RF and CCP antibodies. Although there is overlap in the pathogenesis of PsA and RA, differences are also present that affect the efficacy of treatment. In PsA, levels of interleukin (IL)-1β, IL-6, IL-17, IL-22, IL-23, interferon-γ and tumour necrosis factor-α (TNF-α) are elevated, and in RA, levels of IL-1, IL-6, IL-22, IL-33, TNF-α, chemokine ligand 11 and chemokine C-X-C motif ligand 13 are elevated. Differences in the pathogenesis of RA and PsA translate into some variances in the specificity and efficacy of therapies.
类风湿关节炎(RA)和银屑病关节炎(PsA)在临床表现、影像学表现、合并症及发病机制方面存在关键差异,以此来区分这两种常见的慢性炎症性关节炎。PsA的关节受累通常(但并非总是)不对称,而RA则主要为对称性。无新骨生长的骨侵蚀及颈椎受累是RA的特征,而轴性脊柱受累、银屑病和指甲营养不良是PsA的特征。PsA患者类风湿因子(RF)和抗环瓜氨酸肽(CCP)抗体检测结果通常为阴性,而约80%的RA患者RF和CCP抗体检测结果为阳性。尽管PsA和RA的发病机制存在重叠,但也存在影响治疗效果的差异。在PsA中,白细胞介素(IL)-1β、IL-6、IL-17、IL-22、IL-23、干扰素-γ和肿瘤坏死因子-α(TNF-α)水平升高,而在RA中,IL-1、IL-6、IL-22、IL-33、TNF-α、趋化因子配体11和趋化因子C-X-C基序配体13水平升高。RA和PsA发病机制的差异导致了治疗特异性和疗效的一些差异。