Department of Biomedical Engineering, University of Alberta, 1098 Research Transition Facility, 8308-114 Street, Edmonton, AB, T6G 2V2, Canada.
Department of Medicine, Division of Cardiology, University of Alberta, Edmonton, Canada.
BMC Cancer. 2018 Sep 3;18(1):864. doi: 10.1186/s12885-018-4778-7.
Anthracycline chemotherapy agents are commonly used to treat breast cancer, but also result in cardiac injury, and potentially detrimental effects to vascular and skeletal muscle. Preclinical evidence demonstrates that exercise and caloric restriction can independently reduce anthracycline-related injury to the heart as well as cancer progression, and may be promising short-term strategies prior to treatment administration. For women with breast cancer, a short-term strategy may be more feasible and appealing, as maintaining regular exercise training or a diet throughout chemotherapy can be challenging due to treatment symptoms and psychosocial distress.
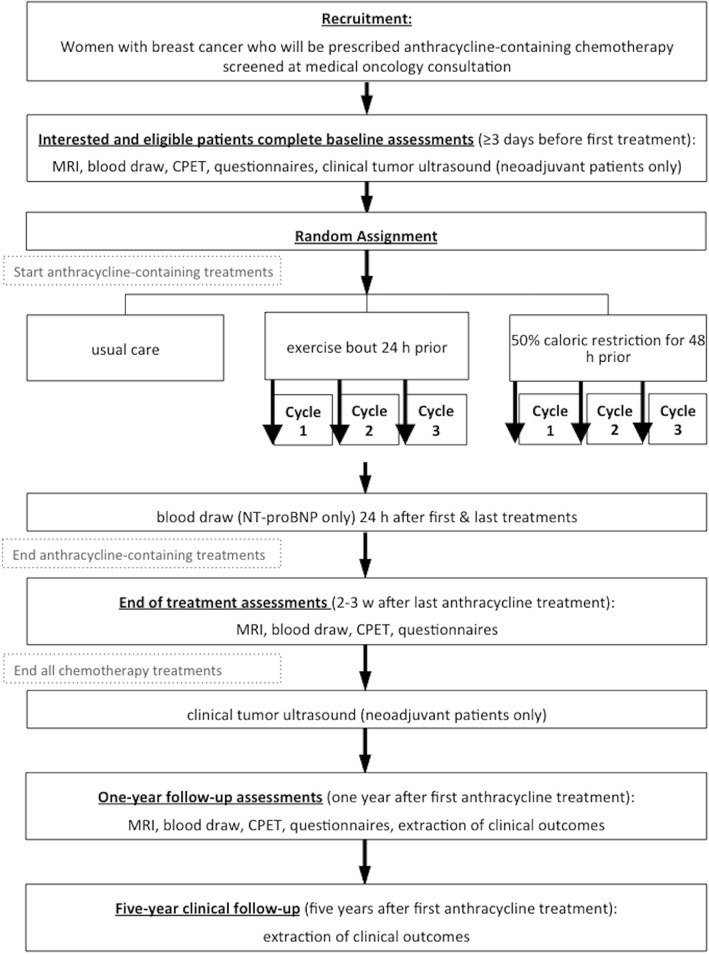
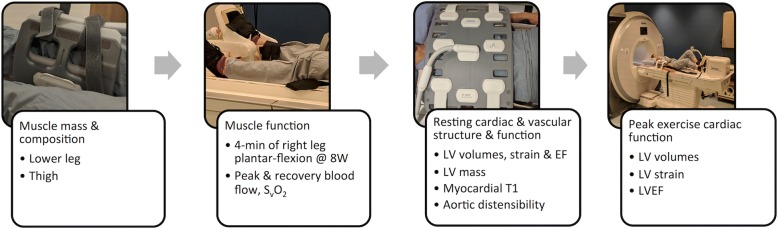
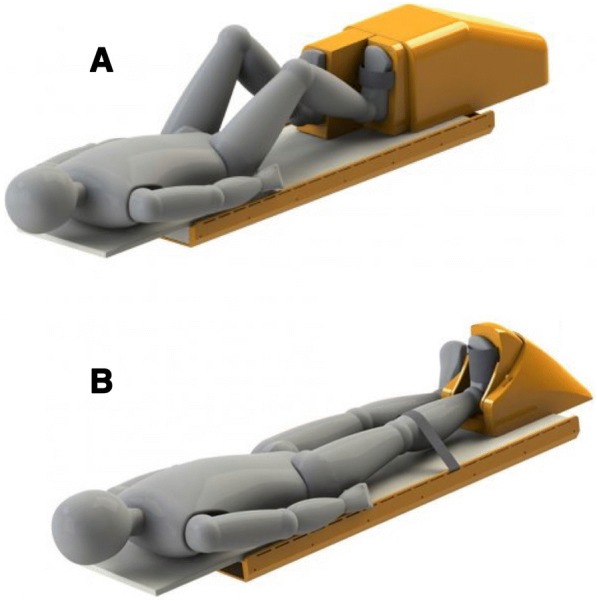
The Caloric Restriction and Exercise protection from Anthracycline Toxic Effects (CREATE) study will determine whether acute application of these interventions shortly prior to receipt of each treatment can reduce anthracycline-related toxicity to the heart, aorta, and skeletal muscle. Fifty-six women with early stage breast cancer scheduled to receive anthracycline treatment will be randomly assigned to one of three groups who will: 1) perform a single, 30-min, vigorous-intensity, aerobic exercise session 24 h prior to each anthracycline treatment; 2) consume a prepared diet reduced to 50% of caloric needs for 48 h prior to each anthracycline treatment; or 3) receive usual cancer care. The primary outcome is magnetic resonance imaging (MRI) derived left ventricular ejection fraction reserve (peak exercise LVEF - resting LVEF) at the end of anthracycline treatment. Secondary outcomes include MRI-derived measures of cardiac, aortic and skeletal muscle structure and function, circulating NT-proBNP, cardiorespiratory fitness and treatment symptoms. Exploratory outcomes include quality of life, fatigue, tumor size (only in neoadjuvant patients), oxidative stress and antioxidants, as well as clinical cardiac or cancer outcomes. MRI, exercise tests, and questionnaires will be administered before, 2-3 weeks after the last anthracycline treatment, and one-year follow-up.
The proposed lifestyle interventions are accessible, low cost, drug-free potential methods for mitigating anthracycline-related toxicity. Reduced toxic effects on the heart, aorta and muscle are very likely to translate to short and long-term cardiovascular health benefits, including enhanced resilience to the effects of subsequent cancer treatment (e.g., radiation, trastuzumab) aging, and infection.
ClinicalTrials.gov NCT03131024; 4/21/18.
蒽环类化疗药物常用于治疗乳腺癌,但也会导致心脏损伤,并对血管和骨骼肌产生潜在的有害影响。临床前证据表明,运动和热量限制可以独立减少蒽环类药物引起的心脏损伤和癌症进展,并且在治疗前应用可能是一种有前途的短期策略。对于患有乳腺癌的女性,短期策略可能更可行和更具吸引力,因为由于治疗症状和心理社会困扰,在整个化疗过程中保持定期运动训练或饮食可能具有挑战性。
热量限制和运动保护免受蒽环类药物毒性作用(CREATE)研究将确定在接受每次治疗前短时间应用这些干预措施是否可以减少蒽环类药物引起的心脏、主动脉和骨骼肌毒性。56 名计划接受蒽环类药物治疗的早期乳腺癌女性将被随机分配到三组中的一组:1)在每次蒽环类药物治疗前 24 小时进行一次 30 分钟剧烈强度的有氧运动;2)在每次蒽环类药物治疗前 48 小时内摄入减少到 50%热量需求的预制饮食;或 3)接受常规癌症护理。主要结局是在蒽环类药物治疗结束时磁共振成像(MRI)得出的左心室射血分数储备(峰值运动 LVEF-静息 LVEF)。次要结局包括 MRI 得出的心脏、主动脉和骨骼肌结构和功能、循环 NT-proBNP、心肺功能和治疗症状的测量值。探索性结局包括生活质量、疲劳、肿瘤大小(仅在新辅助患者中)、氧化应激和抗氧化剂以及临床心脏或癌症结局。在治疗前、最后一次蒽环类药物治疗后 2-3 周以及一年随访时进行 MRI、运动测试和问卷调查。
拟议的生活方式干预措施易于实施、成本低、无需药物,是减轻蒽环类药物相关毒性的潜在方法。心脏、主动脉和肌肉的毒性作用降低很可能转化为短期和长期心血管健康益处,包括增强对后续癌症治疗(例如,辐射、曲妥珠单抗)、衰老和感染的影响的抵抗力。
ClinicalTrials.gov NCT03131024;2018 年 4 月 21 日。