Michael L. Barnett (
Andrew R. Olenski is a graduate student in the Department of Economics at Columbia University, in New York City.
Health Aff (Millwood). 2018 Sep;37(9):1509-1516. doi: 10.1377/hlthaff.2018.0391.
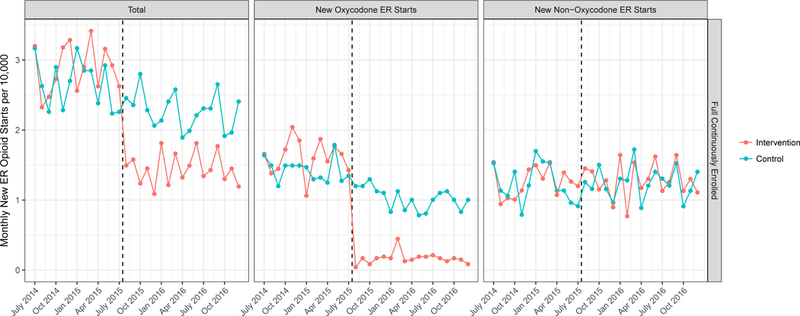
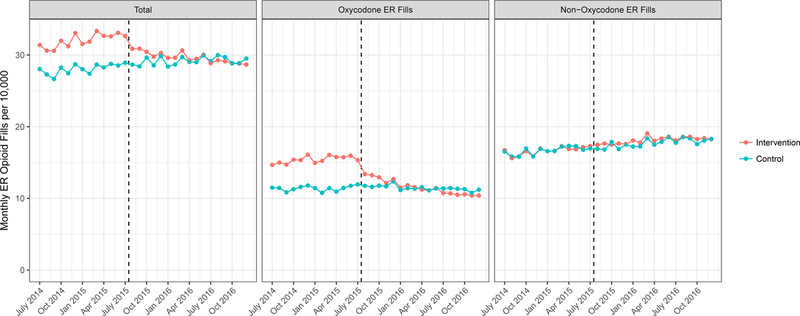
Many insurers are using formulary design to influence opioid prescribing, but it is unclear if these changes lead to reduced use or just substitution between opioids. We evaluated the effect of a new prior authorization process implemented in July 2015 for extended-release (ER) oxycodone by Blue Shield of California. Compared to other commercially insured Californians, among 880,000 Blue Shield enrollees, there was a 36 percent drop in monthly rates of ER opioid initiation relative to control-group members, driven entirely by decreases in ER oxycodone initiation and without any substitution toward other ER opioids. This reduction was offset by a 1.4 percent relative increase in the rate of short-acting opioid fills. There was no significant change in the overall use of any opioids prescribed, measured as morphine milligram equivalents. This suggests that though insurers can play a meaningful role in reducing the prescribing of high-risk ER opioids, a formulary change focused on ER opioids alone is insufficient to decrease total opioid prescribing.
许多保险公司正在利用处方集设计来影响阿片类药物的处方,但是否这些变化会导致使用减少或只是阿片类药物之间的替代尚不清楚。我们评估了加利福尼亚州蓝盾于 2015 年 7 月实施的新的延长释放(ER)羟考酮预先授权流程的效果。与其他商业保险公司承保的加利福尼亚人相比,在 880,000 名蓝盾参保者中,与对照组相比,ER 类阿片类药物的起始使用每月下降了 36%,这完全是由于 ER 羟考酮的起始使用减少所致,而没有向其他 ER 类阿片类药物的任何替代。这一减少被短期阿片类药物填充率相对增加 1.4%所抵消。处方的任何阿片类药物的总体使用量(以吗啡毫克当量衡量)没有显著变化。这表明,尽管保险公司可以在减少高风险 ER 类阿片类药物的处方方面发挥重要作用,但仅针对 ER 类阿片类药物的处方集变化不足以减少总阿片类药物的处方量。