Integrative Oncology - Radiation Biology Unit, BC Cancer Research Centre, 675 West 10th Ave, Vancouver, BC, V5Z 1L3, Canada.
Department of Physics & Astronomy, University of British Columbia, Vancouver, Canada.
Clin Exp Metastasis. 2018 Oct;35(7):691-705. doi: 10.1007/s10585-018-9929-3. Epub 2018 Sep 8.
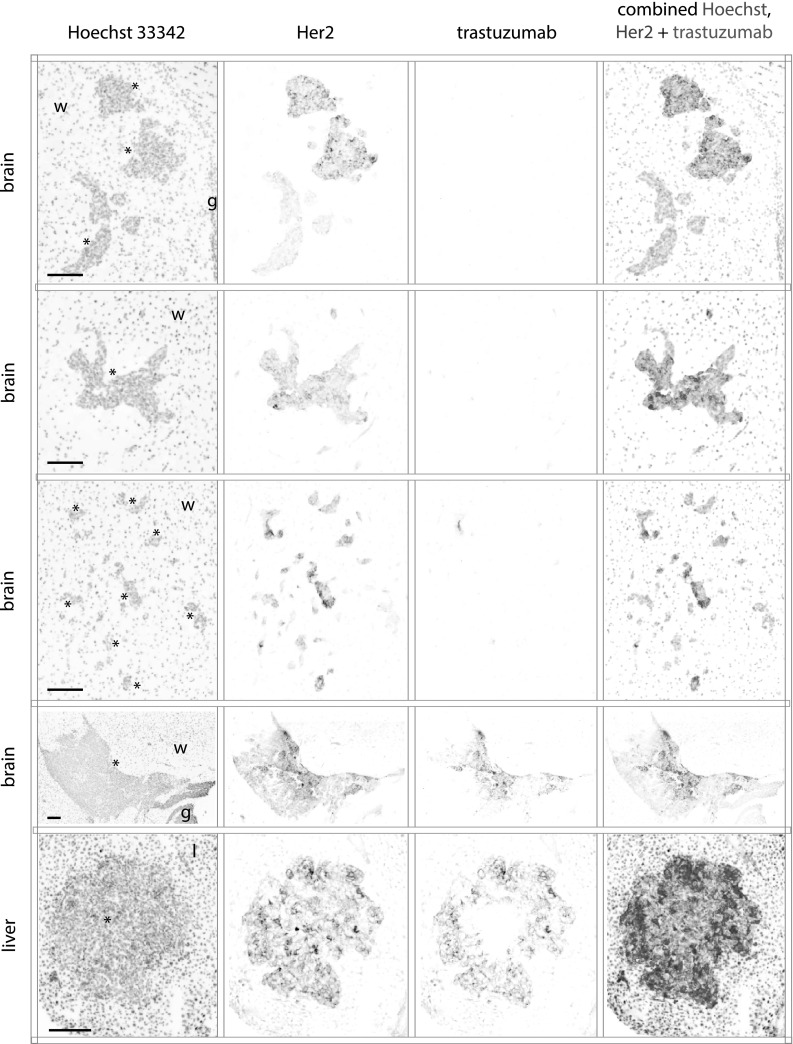
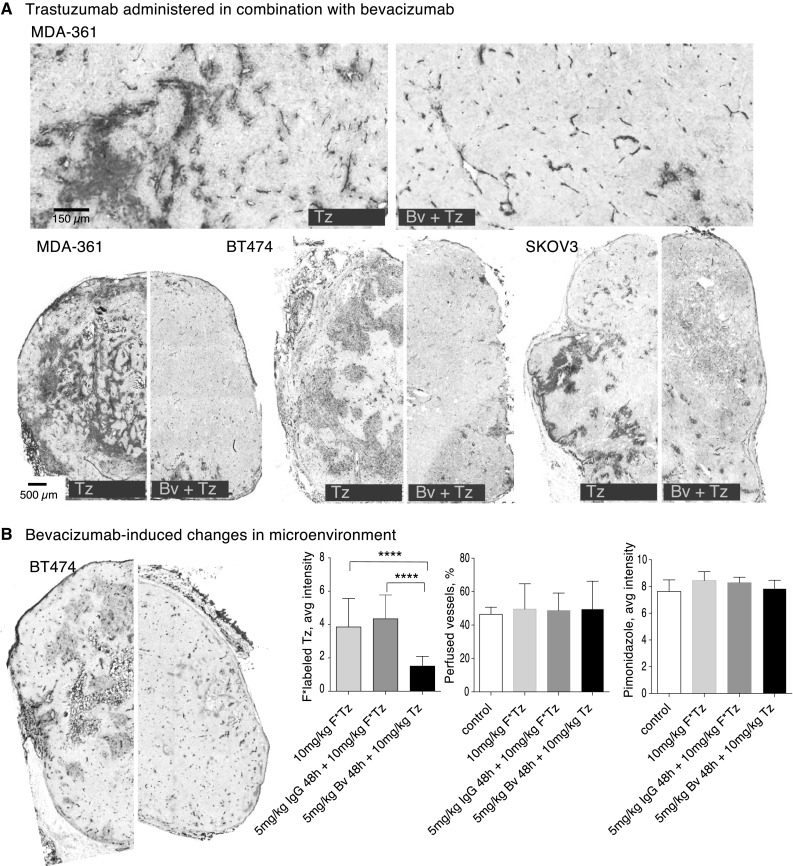
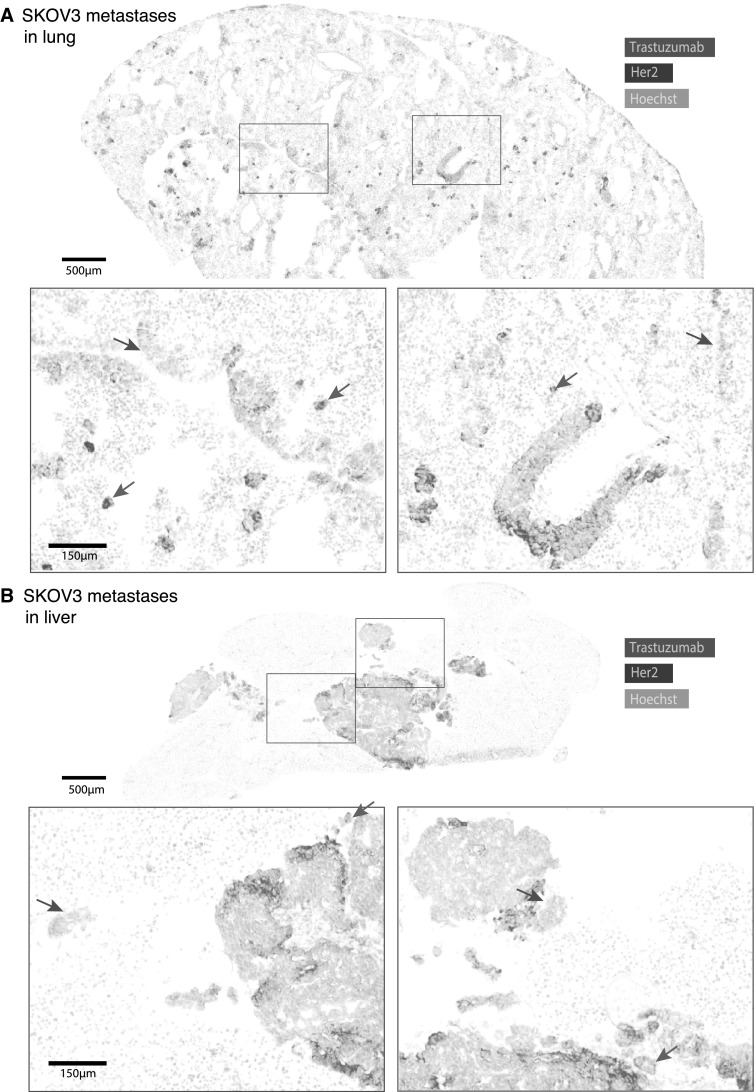
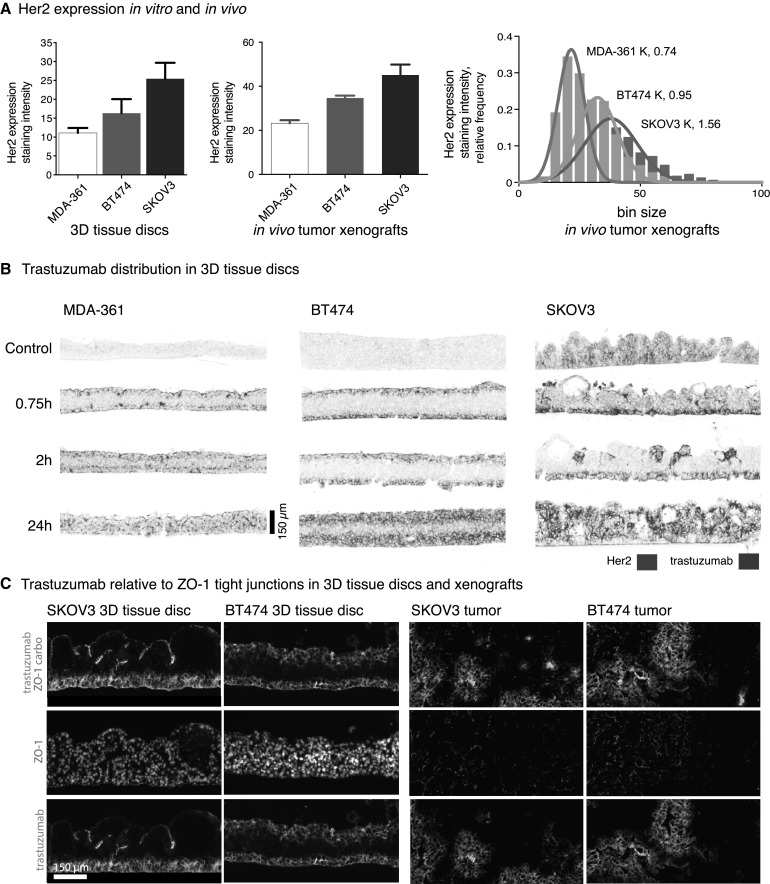
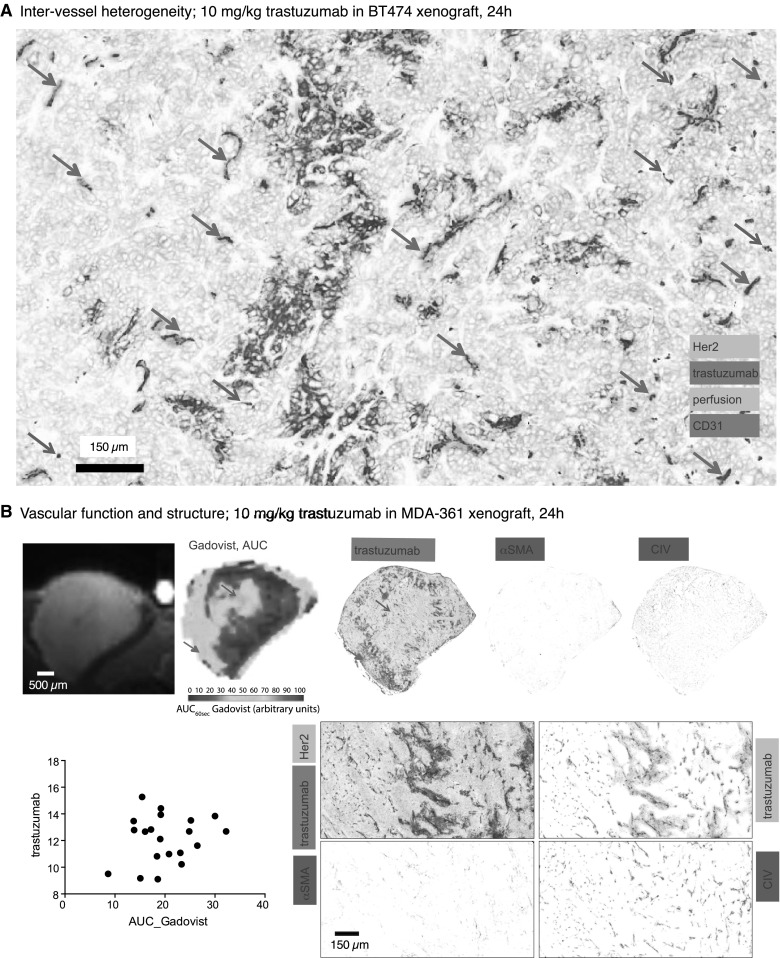
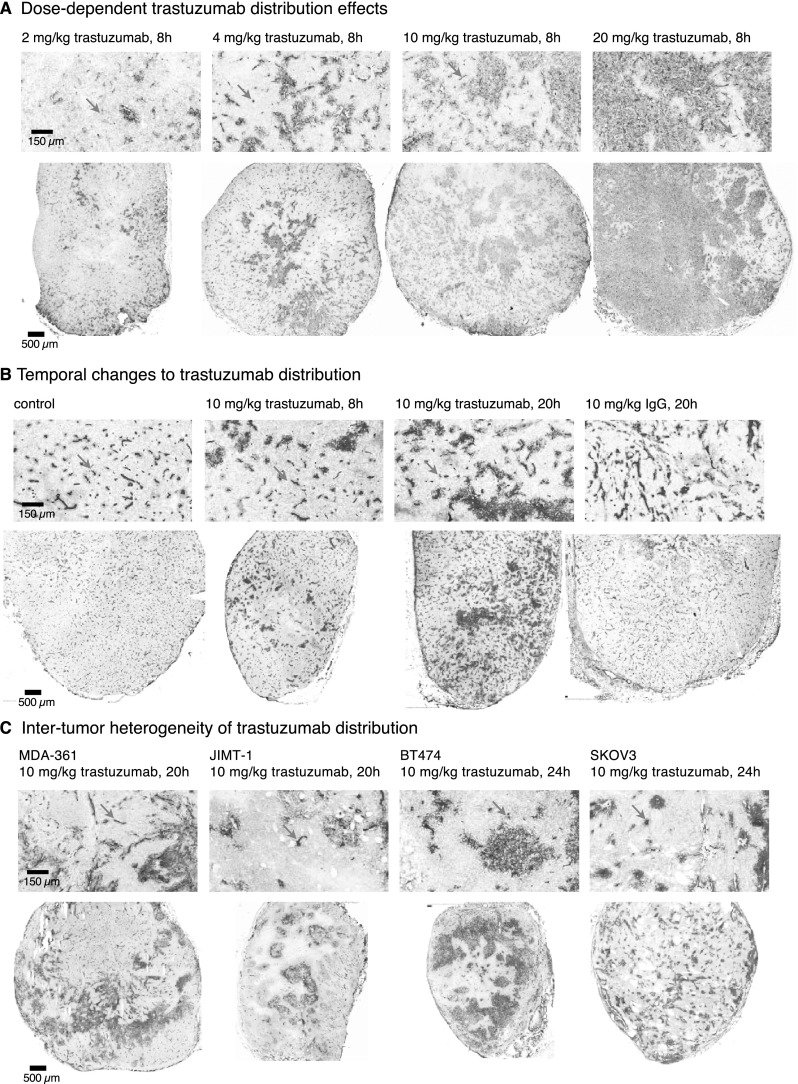
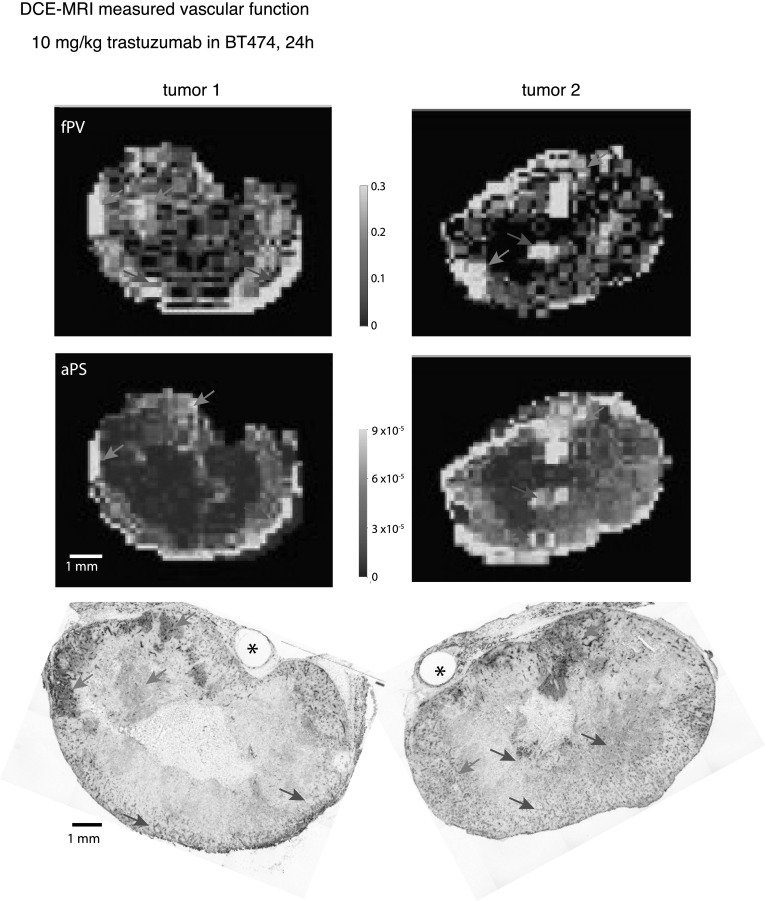
Most HER2-positive metastatic breast cancer patients continue to relapse. Incomplete access to all target HER2-positive cells in metastases and tumor tissues is a potential mechanism of resistance to trastuzumab. The location of locally bound trastuzumab was evaluated in HER2-positive tissues in vivo and as in vivo xenografts or metastases models in mice. Microenvironmental elements of tumors were related to bound trastuzumab using immunohistochemical staining and include tight junctions, vasculature, vascular maturity, vessel patency, hypoxia and HER2 to look for correlations. Trastuzumab was evaluated alone and in combination with bevacizumab. Dynamic contrast-enhanced magnetic resonance imaging parameters of overall vascular function, perfusion and apparent permeability were compared with matched histological images of trastuzumab distribution and vascular patency. Trastuzumab distribution is highly heterogeneous in all models examined, including avascular micrometastases of the brain and lung. Trastuzumab distributes well through the extravascular compartment even in conditions of high HER2 expression and poor convective flow in vivo. Microregional patterns of trastuzumab distribution in vivo do not consistently correlate with vascular density, patency, function or maturity; areas of poor trastuzumab access are not necessarily those with poor vascular supply. The number of vessels with perivascular trastuzumab increases with time and higher doses and dramatically decreases when pre-treated with bevacizumab. Areas of HER2-positive tissue without bound trastuzumab persist in all conditions. These data directly demonstrate tissue- and vessel-level barriers to trastuzumab distribution in vivo that can effectively limit access of the drug to target cells in brain metastases and elsewhere.
大多数 HER2 阳性转移性乳腺癌患者仍会复发。HER2 阳性转移灶和肿瘤组织中无法完全获得所有靶向 HER2 阳性细胞是曲妥珠单抗耐药的潜在机制。在体内 HER2 阳性组织、体内异种移植或转移模型的小鼠中评估了局部结合的曲妥珠单抗的位置。使用免疫组织化学染色,将肿瘤的微环境元素与结合的曲妥珠单抗相关联,包括紧密连接、脉管系统、血管成熟度、血管通畅性、缺氧和 HER2,以寻找相关性。评估了曲妥珠单抗单独使用和与贝伐珠单抗联合使用的效果。对比了整体血管功能、灌注和表观渗透性的动态对比增强磁共振成像参数与匹配的曲妥珠单抗分布和血管通畅性的组织学图像。在所有检查的模型中,包括脑和肺的无血管微转移,曲妥珠单抗的分布高度不均匀。即使在体内 HER2 表达高且对流性较差的情况下,曲妥珠单抗也能很好地分布在血管外间隙中。体内曲妥珠单抗分布的微区模式与血管密度、通畅性、功能或成熟度不一致;药物难以进入的区域不一定是血管供应不良的区域。具有血管周围曲妥珠单抗的血管数量随着时间和较高剂量的增加而增加,并用贝伐珠单抗预处理时则会急剧减少。在所有条件下,没有结合曲妥珠单抗的 HER2 阳性组织区域仍然存在。这些数据直接证明了体内曲妥珠单抗分布的组织和血管水平的屏障,这些屏障可有效地限制药物在脑转移和其他部位的靶细胞中的进入。