Won Young Ju, Lim Byung Gun, Kim Young Sung, Lee Mido, Kim Heezoo
Department of Anesthesiology and Pain Medicine, Korea University Guro Hospital, Korea University College of Medicine, Seoul, Republic of Korea.
J Int Med Res. 2018 Nov;46(11):4386-4398. doi: 10.1177/0300060518796749. Epub 2018 Sep 9.
Previous studies comparing surgical pleth index (SPI)-guided and conventional analgesia have shown differing results. Therefore, we compared the intraoperative opioid requirement, extubation time, postoperative pain scores, and perioperative adverse events between these two modalities.
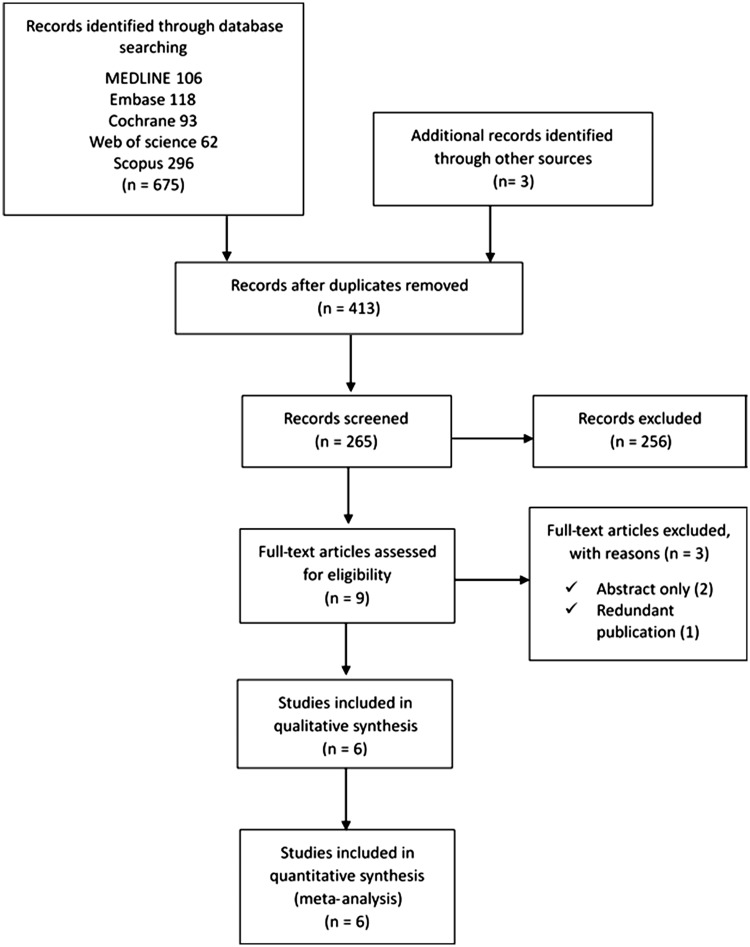
A comprehensive literature search was conducted to identify randomized controlled trials comparing the intraoperative opioid requirement and other outcomes between the two modalities. The mean difference (MD) or the pooled risk ratio and corresponding 95% confidence interval (CI) were used for analysis. A heterogeneity (I) assessment was performed.
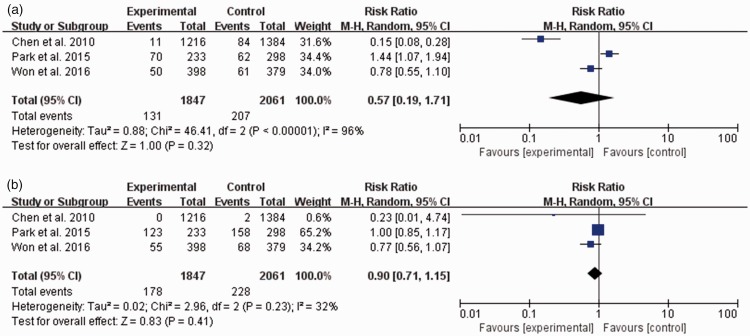
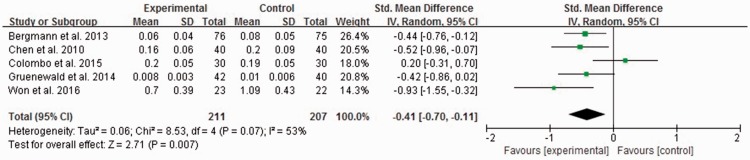
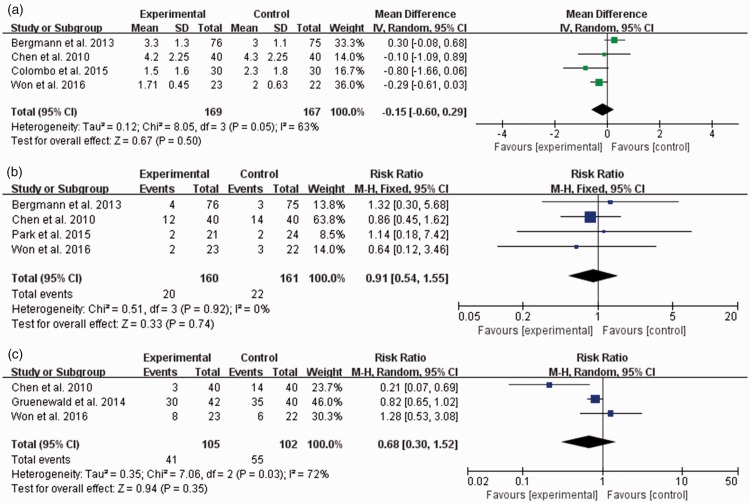
Six randomized controlled trials comparing 463 patients were included. Intraoperative opioid consumption was significantly lower in the SPI-guided than conventional analgesia group (standardized MD, -0.41; 95% CI, -0.70 to -0.11; I = 53%). No significant intergroup difference was observed in the pain score on the first postoperative day or the incidence of perioperative adverse events. The extubation time was considerably shorter in the SPI-guided than conventional analgesia group (MD, -1.91; 95% CI, -3.33 to -0.49; I = 67%).
Compared with conventional analgesia, SPI-guided analgesia can reduce intraoperative opioid consumption and facilitate extubation. Moreover, no intergroup difference was observed in the degree of postoperative pain or incidence of perioperative adverse events.
既往比较手术容积指数(SPI)引导下镇痛与传统镇痛的研究结果各异。因此,我们比较了这两种方式下的术中阿片类药物需求量、拔管时间、术后疼痛评分及围手术期不良事件。
进行全面的文献检索,以确定比较两种方式下术中阿片类药物需求量及其他结果的随机对照试验。采用平均差(MD)或合并风险比及相应的95%置信区间(CI)进行分析。进行异质性(I)评估。
纳入6项比较463例患者的随机对照试验。SPI引导下镇痛组的术中阿片类药物消耗量显著低于传统镇痛组(标准化MD,-0.41;95%CI,-0.70至-0.11;I = 53%)。术后第1天的疼痛评分或围手术期不良事件发生率在组间未观察到显著差异。SPI引导下镇痛组的拔管时间比传统镇痛组明显更短(MD,-1.91;95%CI,-3.33至-0.49;I = 67%)。
与传统镇痛相比,SPI引导下镇痛可减少术中阿片类药物消耗并促进拔管。此外,术后疼痛程度或围手术期不良事件发生率在组间未观察到差异。