Rawala Muhammad Shabbir, Khaliq Muhammad Farhan, Iqbal Muhammad Asif, Naqvi S Tahira Shah, Farhan Kinaan, Myers Andrew, Helmick Kristen
Department of Medicine, Charleston Area Medical Center, Charleston, WV, USA.
Department of Medicine, Jinnah Medical and Dental College, Karachi, Pakistan.
Case Rep Pulmonol. 2018 Aug 19;2018:9830797. doi: 10.1155/2018/9830797. eCollection 2018.
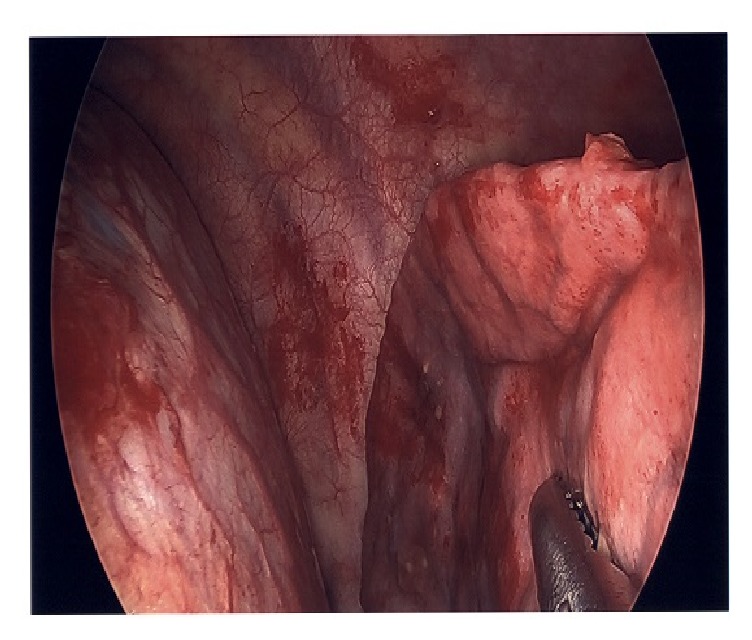
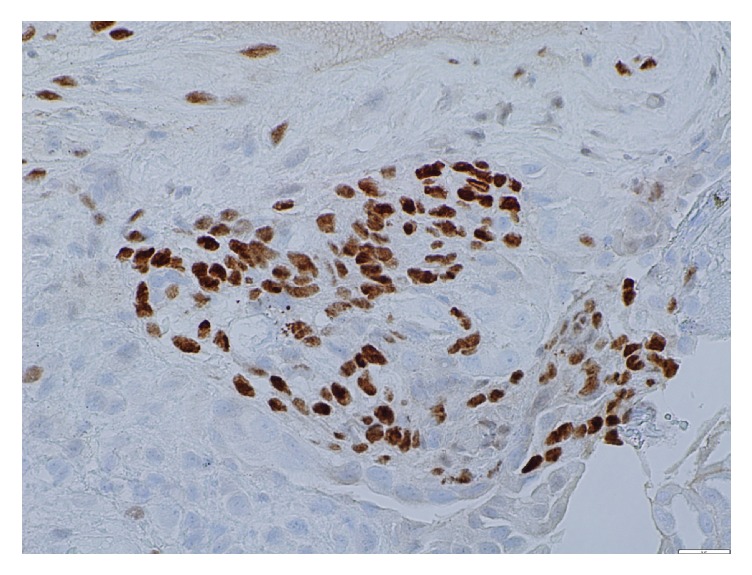
Endometriosis is a common condition in which endometrial cells and stroma are deposited in extrauterine sites. Its prevalence has been estimated to be 10% of reproductive age females. It is commonly found in the pelvis; however, it may be found in the abdomen, thorax, brain, or skin. Thoracic involvement is a relatively rare presentation of this common disease. Thoracic endometriosis commonly presents as pneumothorax in 73% of patients. A rarer presentation of thoracic endometriosis is hemothorax (<14%) or hemoptysis (7%). Thoracic endometriosis is an uncommon cause of a pleural effusion. We present a case of 28-year-old African American female with no other medical conditions. She presented to the hospital with worsening right-sided pleuritic chest pain, dyspnea, and menorrhagia. She had been complaining of pleuritic chest pain for 5 years, the onset of which corresponds to the start of her menstrual cycle and is relieved with cessation of menses. Initial laboratory studies revealed a severe microcytic anemia with normal coagulation profile. Chest X-ray showed small right pleural effusion and suspicious for airspace disease. A computed tomography (CT) of chest was ordered for further clarification and identified large right pleural effusion. CT-guided thoracentesis removed 500 ml of serosanguinous fluid consisting of blood elements. There can be multiple sites involved with endometriosis and can present with wide range of symptoms that occur periodically with menses in young woman. The history and pleural fluid findings of this case are suggestive of Thoracic Endometriosis Syndrome. The diagnosis of this is often missed or delayed by clinicians, which can result in recurrent hospitalization and other complications. As internists we should be suspicious of atypical presentations of endometriosis and treat them early before complications develop. This case also highlights the importance of suspecting atypical etiologies for pleural effusion.
子宫内膜异位症是一种常见病症,其中子宫内膜细胞和间质沉积于子宫外部位。据估计,其在育龄女性中的患病率为10%。它常见于盆腔;然而,也可能出现在腹部、胸部、脑部或皮肤。胸部受累是这种常见疾病相对罕见的表现形式。胸部子宫内膜异位症在73%的患者中通常表现为气胸。胸部子宫内膜异位症较罕见的表现形式是血胸(<14%)或咯血(7%)。胸部子宫内膜异位症是胸腔积液的罕见病因。我们报告一例28岁无其他疾病的非裔美国女性病例。她因右侧胸膜炎性胸痛、呼吸困难和月经过多入院。她主诉胸膜炎性胸痛已有5年,胸痛发作与月经周期开始相对应,月经停止后缓解。初始实验室检查显示严重小细胞贫血,凝血指标正常。胸部X线显示右侧少量胸腔积液,怀疑有空洞性病变。因此安排了胸部计算机断层扫描(CT)以进一步明确,结果发现右侧大量胸腔积液。CT引导下胸腔穿刺抽出5ml由血液成分组成的浆液性血性液体。子宫内膜异位症可累及多个部位,年轻女性可出现多种与月经周期周期性相关的症状。该病例的病史和胸腔积液检查结果提示为胸腔子宫内膜异位症综合征。临床医生常常漏诊或延误该疾病的诊断,这可能导致反复住院及其他并发症。作为内科医生,我们应怀疑子宫内膜异位症的非典型表现,并在并发症出现前尽早进行治疗。该病例还凸显了怀疑胸腔积液非典型病因的重要性。