Cho Ara, Jantschitsch Christian, Knobler Robert
Department of Dermatology, Medizinische Universität Wien, Vienna, Austria.
Front Med (Lausanne). 2018 Aug 27;5:236. doi: 10.3389/fmed.2018.00236. eCollection 2018.
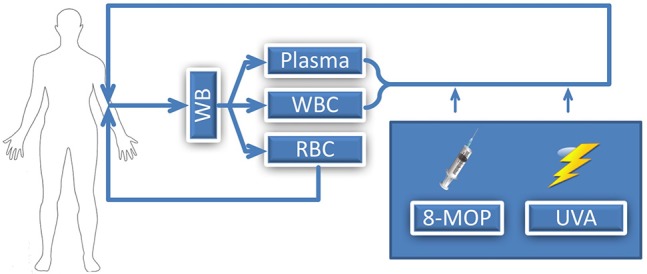
Extracorporeal photopheresis (ECP) has been in clinical use for over three decades after receiving FDA approval for the palliative treatment of the Sézary Syndrome variant of cutaneous T-cell lymphoma (CTCL) in 1988. After the first positive experiences with CTCL, additional indications have been successfully explored including areas such as graft-vs.-host disease (GVHD), scleroderma, and solid organ transplantation. The mechanism of action is still not fully resolved, but important steps in understanding ECP in recent years have been very informative. Originally, the primary hypothesis stated that psoralen and ultraviolet A (UVA) in combination induce apoptosis in the treated immune cells. This view shifted in favor of dendritic cell initiation, modification of the cytokine profile and stimulation of several T-cell lineages, in particular regulatory T-cells. A number of ECP guidelines have been produced to optimize treatment regimens in the clinical context. In CTCL, enough evidence is available for the use of ECP as a first line treatment for Sézary Syndrome (SS), but also as a second line or rescue treatment in therapy-refractory forms of mycosis fungoides (MF). ECP in the treatment of acute and chronic GVHD has shown promising results as second line therapy in steroid-refractory presentations. In solid organ transplantation, ECP has been used to increase tissue tolerance and decrease infections with opportunistic pathogens, attributed to the use of high doses of immunosuppressive medication. Infection with cytomegalovirus (CMV) remains a limiting factor affecting survival in solid organ transplantation and the role of ECP will be discussed in this review. A trend toward prophylactic use of ECP can be observed and may further contribute to improve the outcome in many patients. To further deepen our knowledge of ECP and thus facilitate its use in patients that potentially benefit most from it, future prospective randomized trials are urgently needed in this rapidly growing field. The aim of this review is to (1) introduce the method, (2) give an overview where ECP has shown promising effects and has become an essential part of treatment protocols, and (3) to give recommendations on how to proceed in numerous indications.
体外光化学疗法(ECP)自1988年获得美国食品药品监督管理局(FDA)批准用于皮肤T细胞淋巴瘤(CTCL)的Sezary综合征变体的姑息治疗以来,已在临床应用超过三十年。在CTCL取得首批积极经验后,人们成功探索了其他适应症,包括移植物抗宿主病(GVHD)、硬皮病和实体器官移植等领域。其作用机制尚未完全明确,但近年来在理解ECP方面取得的重要进展提供了很多有价值的信息。最初,主要假说是补骨脂素和紫外线A(UVA)联合作用可诱导被治疗免疫细胞凋亡。这种观点后来转向支持树突状细胞的启动、细胞因子谱的改变以及对多个T细胞谱系(特别是调节性T细胞)的刺激。为了在临床环境中优化治疗方案,已制定了一些ECP指南。在CTCL中,有足够的证据表明ECP可作为Sezary综合征(SS)的一线治疗方法,也可作为蕈样肉芽肿(MF)治疗难治形式的二线或挽救治疗方法。ECP在治疗急性和慢性GVHD方面已显示出有希望的结果,可作为类固醇难治性表现的二线治疗方法。在实体器官移植中,由于使用了高剂量免疫抑制药物,ECP已被用于提高组织耐受性并减少机会性病原体感染。巨细胞病毒(CMV)感染仍然是影响实体器官移植患者生存的一个限制因素,本文将讨论ECP在这方面的作用。可以观察到一种预防性使用ECP的趋势,这可能会进一步有助于改善许多患者的治疗结果。为了进一步加深我们对ECP的了解,从而促进其在可能最受益的患者中的应用,在这个快速发展的领域迫切需要未来的前瞻性随机试验。本综述的目的是:(1)介绍该方法;(2)概述ECP已显示出有希望的效果并已成为治疗方案重要组成部分的领域;(3)就如何在众多适应症中开展治疗提出建议。