Ibrahim Mustafa E, Chang Cara, Hu Yichun, Hogan Susan L, Mercke Nickie, Gomez Madeleine, O'Bryant Cindy L, Bowles Daniel W, George Blessy, Wen Xia, Buckley Brian, Aleksunes Lauren, Joy Melanie S
Department of Pharmaceutical Sciences, Skaggs School of Pharmacy and Pharmaceutical Sciences, University of Colorado, Anschutz Medical Campus, 12850 E. Montview Blvd, Mail Stop C238, Room V20-4108, Aurora, CO, 80045, USA.
Kidney Center, University of North Carolina School of Medicine, Division of Nephology and Hypertension, Chapel Hill, NC, 27516, USA.
Eur J Clin Pharmacol. 2019 Jan;75(1):51-57. doi: 10.1007/s00228-018-2552-z. Epub 2018 Sep 15.
The ability to predict and detect clinical and subclinical nephrotoxicity early in the course of therapy has the potential to improve long-term outcomes in cancer patients receiving cisplatin chemotherapy. Pharmacokinetic parameters could serve as predictors of cisplatin-induced nephrotoxicity.
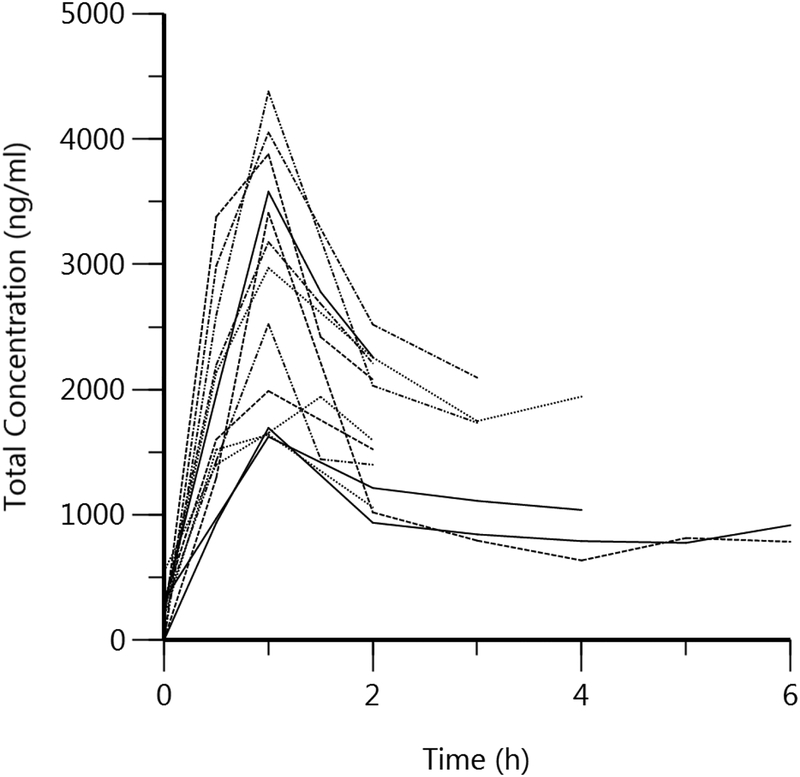
Participants [n = 13] were treated with a 1-h cisplatin infusion [30-75 mg/m]. Blood was collected pre-dose and up to 6 h post-dose. Urinary biomarkers [KIM-1, calbindin, clusterin, GST-pi, β2M, albumin, NGAL, osteopontin, clusterin, MCP-1, cystatin C, and TFF3] were measured at baseline, days 3 and 10. Total and unbound platinum concentrations were measured using ICP/MS. Noncompartmental analysis was performed, and correlation and regression analyses evaluated the relationships between platinum pharmacokinetics and nephrotoxicity.
Peak platinum urinary concentrations correlated with urinary levels of KIM-1, calbindin, clusterin, GST-pi, β2M, albumin, NGAL, osteopontin, clusterin, cystatin C, and TFF3 at day 10. Unbound platinum plasma concentrations at 2 h also correlated with urinary clusterin, β2M, cystatin C, NGAL, osteopontin, and TFF3 at day 3. Regression analyses suggested 2-h total plasma platinum concentrations greater than 2000 ng/ml, and peak urinary platinum concentrations above 24,000 ng/ml may serve as potential approximations for elevated risk of nephrotoxicity. Platinum area under the plasma concentration time curve was associated with serum creatinine and estimated glomerular filtration rate.
Peak plasma and urinary platinum concentrations and pharmacokinetic parameters were associated with risk of subclinical cisplatin-induced kidney injury as assessed using novel urinary biomarkers. Future studies will examine these relationships in larger clinical populations of cisplatin-induced acute kidney injury.
在接受顺铂化疗的癌症患者治疗过程中,早期预测和检测临床及亚临床肾毒性的能力有可能改善其长期预后。药代动力学参数可作为顺铂诱导肾毒性的预测指标。
13名参与者接受1小时的顺铂输注(30 - 75mg/m²)。给药前及给药后6小时内采集血液。在基线、第3天和第10天测量尿液生物标志物(KIM-1、钙结合蛋白、簇集蛋白、谷胱甘肽S-转移酶π、β2微球蛋白、白蛋白、中性粒细胞明胶酶相关脂质运载蛋白、骨桥蛋白、簇集蛋白、单核细胞趋化蛋白-1、胱抑素C和三叶因子3)。使用电感耦合等离子体质谱法测量总铂和游离铂浓度。进行非房室分析,相关性和回归分析评估铂药代动力学与肾毒性之间的关系。
第10天,铂尿峰值浓度与KIM-1、钙结合蛋白、簇集蛋白、谷胱甘肽S-转移酶π、β2微球蛋白、白蛋白、中性粒细胞明胶酶相关脂质运载蛋白、骨桥蛋白、簇集蛋白、胱抑素C和三叶因子3的尿水平相关。第3天,2小时时的游离铂血浆浓度也与尿簇集蛋白、β2微球蛋白、胱抑素C、中性粒细胞明胶酶相关脂质运载蛋白、骨桥蛋白和三叶因子3相关。回归分析表明,2小时时总血浆铂浓度大于2000ng/ml以及尿铂峰值浓度高于24000ng/ml可能是肾毒性风险升高的潜在近似指标。血浆浓度时间曲线下的铂面积与血清肌酐和估计肾小球滤过率相关。
血浆和尿铂峰值浓度及药代动力学参数与使用新型尿生物标志物评估的亚临床顺铂诱导肾损伤风险相关。未来研究将在更大的顺铂诱导急性肾损伤临床人群中研究这些关系。