Michel Alain, Pladys Adelaide, Bayat Sahar, Couchoud Cécile, Hannedouche Thierry, Vigneau Cécile
CHU Pontchaillou, Service de néphrologie, 2 rue H Le Guilloux, 35033, Rennes cedex, France.
EHESP, Département d'Epidémiologie et de Biostatistiques, Rennes, France.
BMC Nephrol. 2018 Sep 17;19(1):233. doi: 10.1186/s12882-018-1036-9.
Emergency start (ES) of dialysis has been associated with worse outcome, but remains poorly documented. This study aims to compare the profile and outcome of a large cohort of patients starting dialysis as an emergency or as a planned step in France.
Data on all patients aged 18 years or older who started dialysis in mainland France in 2012 or in 2006 were collected from the Renal Epidemiology and Information Network and compared, depending on the dialysis initiation condition: ES or Planned Start (PS). ES was defined as a first dialysis within 24 h after a nephrology visit due to a life-threatening event. Three-year survival were compared, and a multivariate model was performed after multiple imputation of missing data, to determine the parameters independently associated with three-year survival.
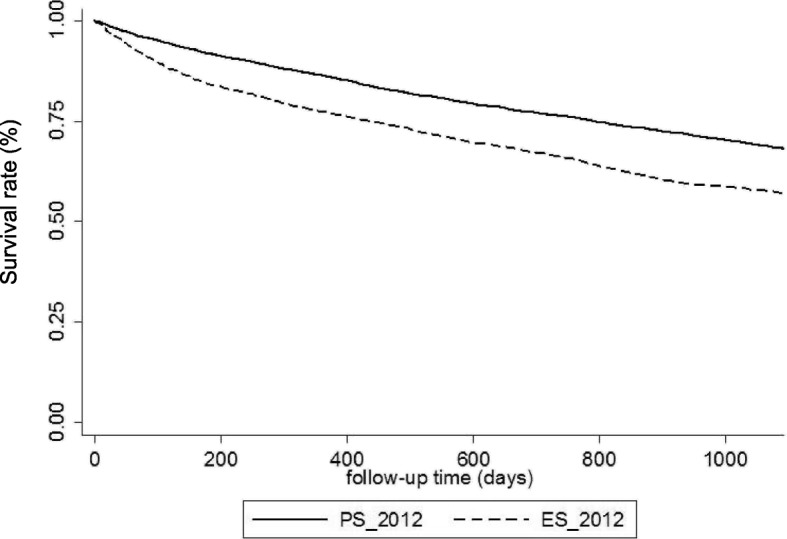
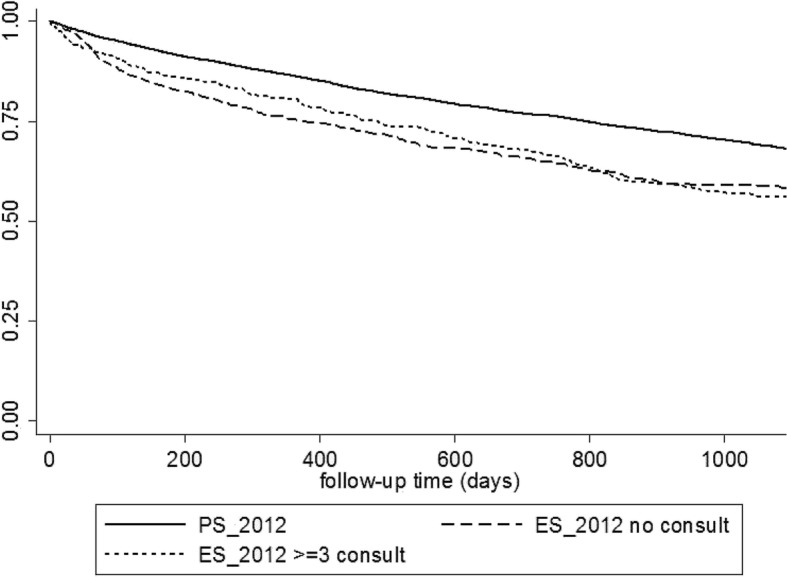
In 2012, 30.3% of all included patients (n = 8839) had ES. Comorbidities were more frequent in the ES than PS group (≥ 2 cardiovascular diseases: 39.2% vs 28.8%, p < 0.001). ES was independently associated with worse three-year survival (57% vs. 68.2%, p = 0.029, HR 1.10, 95% CI 1.01-1.19) in multivariate analysis. Among ES group, a large part had a consistent previous follow-up: 36.4% of them had ≥3 nephrology consultations in the previous year. This subgroup of patients had a particularly high comorbidity burden. ES rate was stable between 2006 and 2012, but some proactive regions succeeded in reducing markedly the ES rate.
ES remains frequent and is independently associated with worse three-year survival, demonstrating that ES deleterious impact is never overcome. This study shows that a large part of patients with ES had a previous follow-up, but high comorbidity burden that could favor acute decompensation with life-threatening conditions before uremic symptoms appearance. This suggests the need of closer end-stage renal disease follow-up or early dialysis initiation in these high-risk patients.
急诊开始透析(ES)与较差的预后相关,但相关记录仍然很少。本研究旨在比较法国一大群以急诊或计划方式开始透析的患者的特征和预后。
收集2012年或2006年在法国大陆开始透析的所有18岁及以上患者的数据,这些数据来自肾脏流行病学和信息网络,并根据透析开始情况进行比较:急诊开始(ES)或计划开始(PS)。ES被定义为因危及生命的事件在肾病科就诊后24小时内进行的首次透析。比较三年生存率,并在对缺失数据进行多次插补后进行多变量模型分析,以确定与三年生存率独立相关的参数。
2012年,所有纳入患者(n = 8839)中有30.3%为急诊开始透析。急诊开始透析组的合并症比计划开始透析组更常见(≥2种心血管疾病:39.2%对28.8%,p < 0.001)。在多变量分析中,急诊开始透析与较差的三年生存率独立相关(57%对68.2%,p = 0.029,HR 1.10,95%CI 1.01 - 1.19)。在急诊开始透析组中,很大一部分患者之前有持续的随访:其中36.4%的患者在前一年有≥3次肾病科会诊。这一亚组患者的合并症负担特别高。2006年至2012年期间,急诊开始透析率保持稳定,但一些积极主动的地区成功地显著降低了急诊开始透析率。
急诊开始透析仍然很常见,并且与较差的三年生存率独立相关,表明急诊开始透析的有害影响从未被克服。本研究表明,很大一部分急诊开始透析的患者之前有随访,但合并症负担高,这可能在尿毒症症状出现之前就有利于急性失代偿并伴有危及生命的情况。这表明需要对这些高危患者进行更密切的终末期肾病随访或更早开始透析。