Department of Medical Laboratory Sciences, School of Biomedical & Allied Health Sciences, College of Health Sciences, University of Ghana, P.O. Box KB 143, Korle Bu, Accra, Ghana.
Department of Virology, Noguchi Memorial Institute for Medical Research, College of Health Sciences, University of Ghana, Legon, Accra, Ghana.
Virol J. 2018 Sep 17;15(1):143. doi: 10.1186/s12985-018-1051-2.
Antiretrovirals have been available in Ghana since 2003 for HIV-1 positive pregnant women for prevention of mother-to-child transmission (PMTCT). Suboptimal responses to treatment observed post-PMTCT interventions necessitated the need to investigate the profile of viral mutations generated. This study investigated HIV-1 drug resistance profiles in mothers in selected centres in Ghana on treatment with a history of prophylaxis.
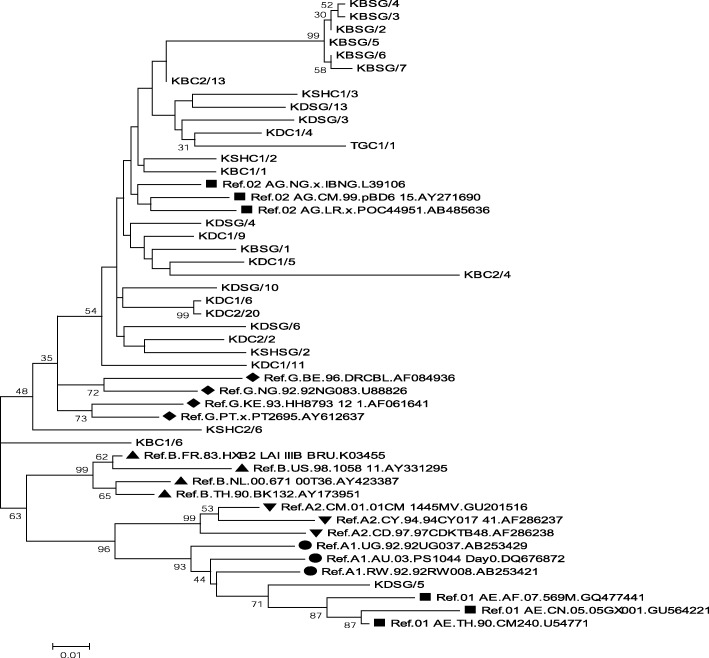
Genotypic Drug Resistance Testing for HIV-1 was carried out. Subtyping was done by phylogenetic analysis and Stanford HIV Database programme was used for drug resistance analysis and interpretation. To compare the significance between the different groups and the emergence of drug resistance mutations, p values were used.
Participants who had prophylaxis before treatment, those who had treatment without prophylaxis and those yet to initiate PMTCT showed 32% (8), 5% (3) and 15% (4) HIV-1 drug resistance associated mutations respectively. The differences were significant with p value < 0.05. Resistance Associated Mutations (RAMs) were seen in 14 participants (35%) to nucleoside reverse transcriptase inhibitors (NRTIs) and non-nucleoside reverse transcriptase inhibitors (NNRTIs). The most common NRTI mutation found was M184 V; K103 N and A98G were the most common NNRTI mutations seen. Thymidine Analogue Mutations (TAMs) such as M41 L, K70R and T215Y were found in all the groups; the most common of the TAMs found were M41 L and T215Y. Majority of the subtypes were CRF02_AG (82%).
In Ghana initiation of uninterrupted treatment upon diagnosis, coupled with drug resistance testing, would produce a better treatment outcome for HIV-1 positive pregnant women.
自 2003 年以来,加纳已经为 HIV-1 阳性孕妇提供了抗逆转录病毒药物,用于预防母婴传播(PMTCT)。在 PMTCT 干预措施之后观察到的治疗反应不理想,需要调查产生的病毒突变特征。本研究调查了加纳选定中心接受治疗且有预防史的母亲的 HIV-1 耐药情况。
进行了 HIV-1 基因型耐药性检测。通过系统发育分析进行亚型分类,使用斯坦福 HIV 数据库程序进行耐药性分析和解释。为了比较不同组之间的差异和耐药突变的出现,使用了 p 值。
接受治疗前有预防措施、未接受预防措施但已开始 PMTCT 以及尚未开始 PMTCT 的参与者中,HIV-1 耐药相关突变的发生率分别为 32%(8 例)、5%(3 例)和 15%(4 例)。差异具有统计学意义(p 值<0.05)。14 名参与者(35%)出现了核苷类逆转录酶抑制剂(NRTIs)和非核苷类逆转录酶抑制剂(NNRTIs)的耐药相关突变。最常见的 NRTI 突变是 M184V;最常见的 NNRTI 突变是 K103N 和 A98G。所有组中均发现了胸腺嘧啶类似物突变(TAMs),如 M41L、K70R 和 T215Y;最常见的 TAMs 是 M41L 和 T215Y。大多数亚型是 CRF02_AG(82%)。
在加纳,一旦确诊即开始不间断治疗,并结合耐药性检测,将为 HIV-1 阳性孕妇提供更好的治疗效果。