Division of Urology, Department of Surgery, Brigham and Women's Hospital, Harvard Medical School, Boston, Massachusetts.
Department of Biostatistics and Computational Biology, Dana-Farber Cancer Institute, Boston, Massachusetts.
Mol Cancer Res. 2019 Jan;17(1):263-276. doi: 10.1158/1541-7786.MCR-18-0412. Epub 2018 Sep 17.
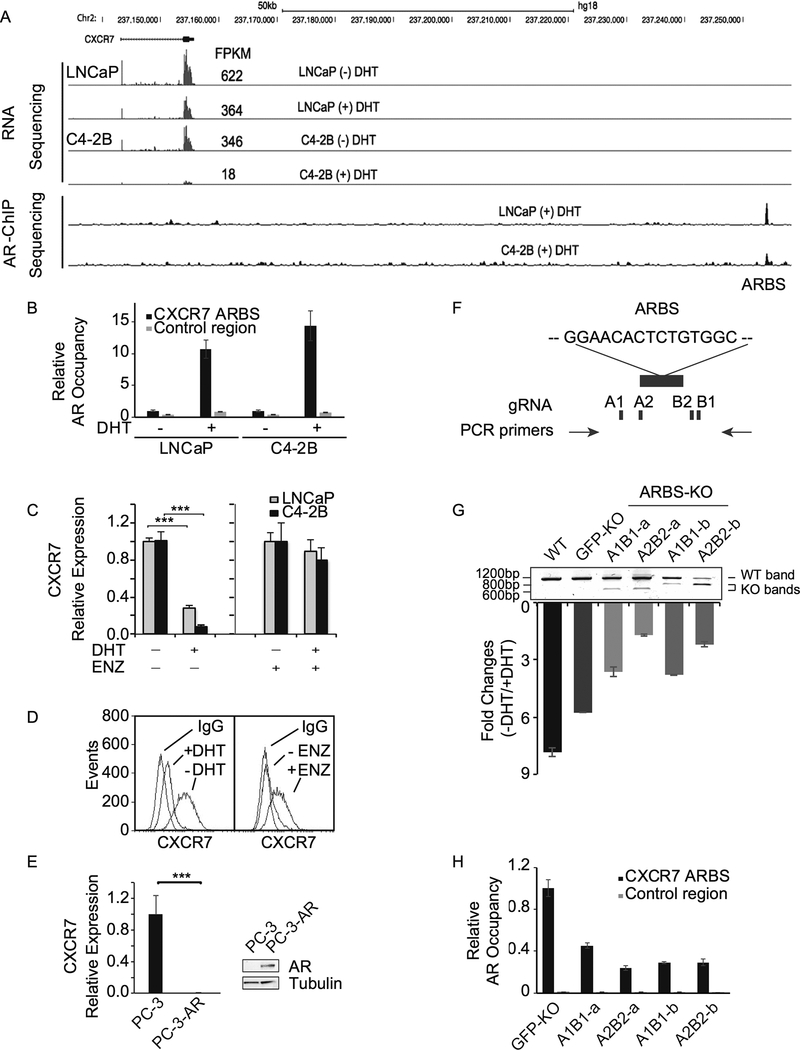
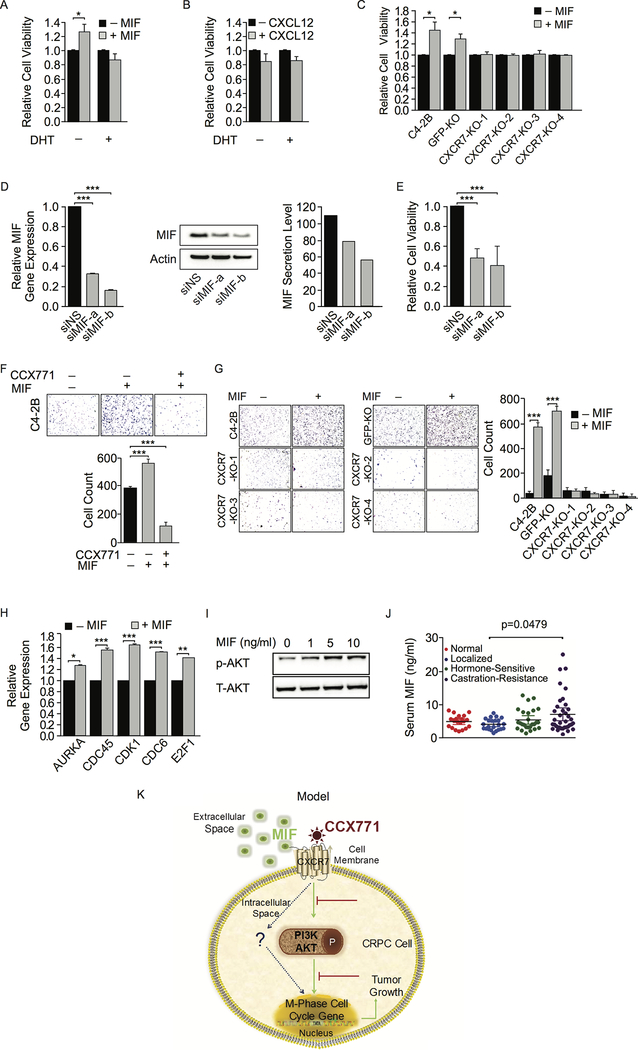
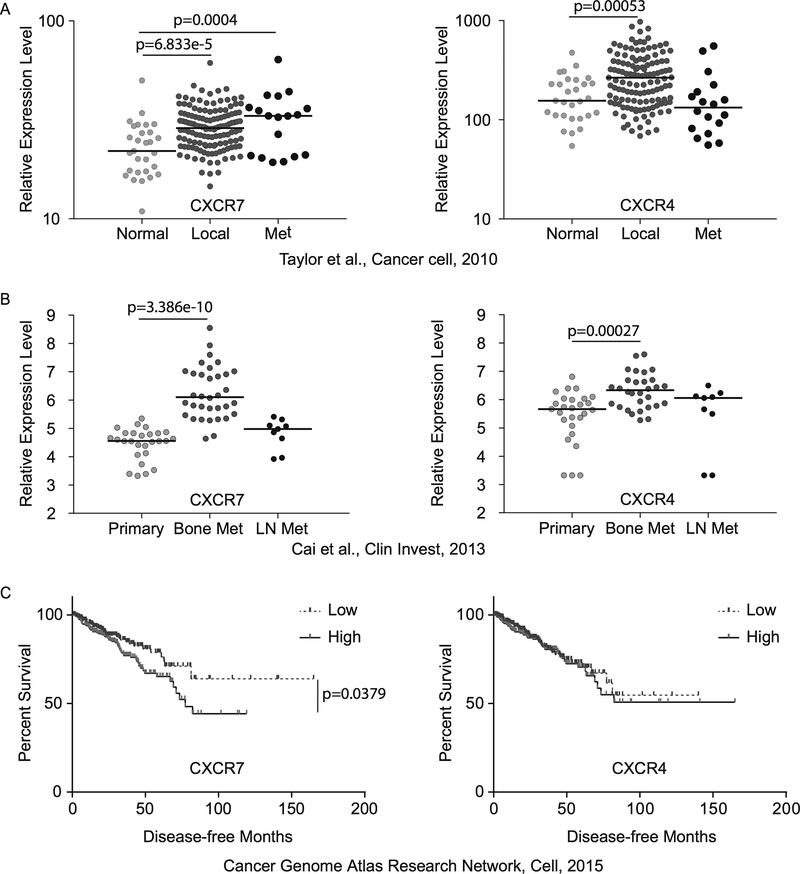
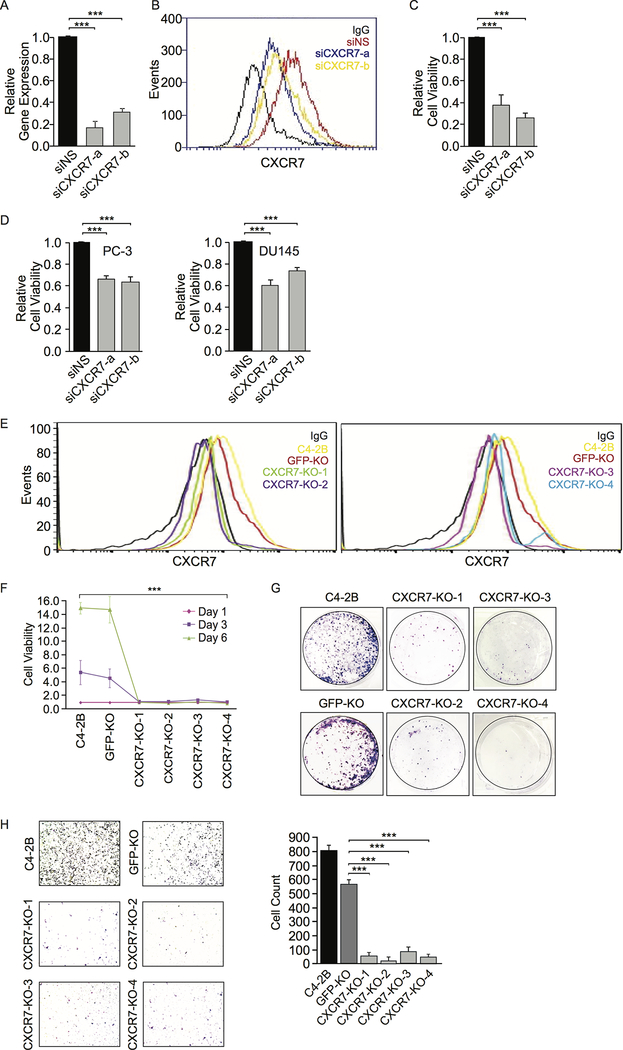
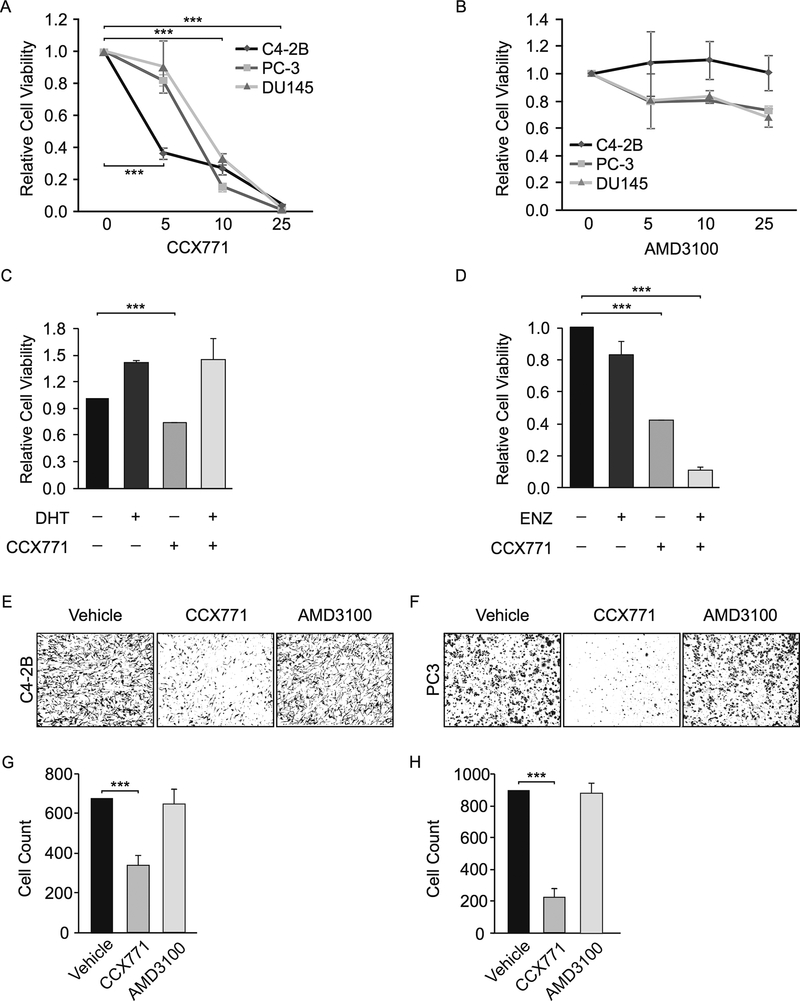
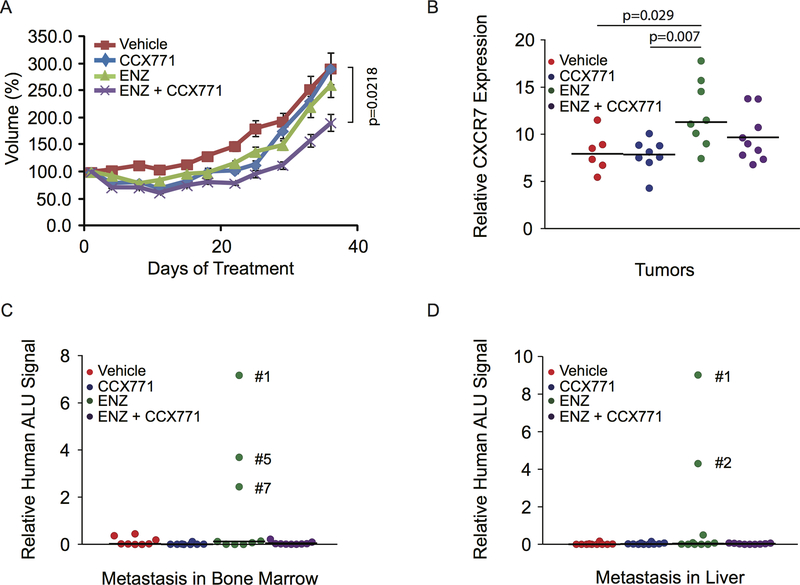
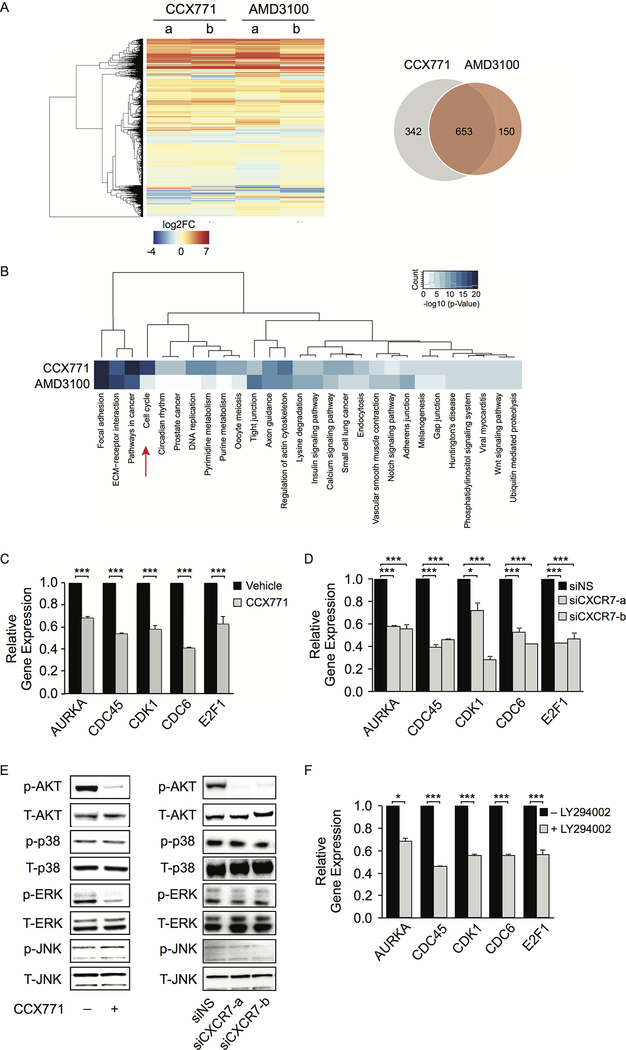
Although androgen deprivation therapy (ADT) is an effective treatment for metastatic prostate cancer, incurable castration-resistant prostate cancer (CRPC) inevitably develops. Importantly, androgen receptor (AR) continues to be critical for prostate cancer growth and progression after ADT. One of the underlying molecular mechanisms is derepression of AR-repressed genes involved in cell cycle and proliferation after ADT. Here, the data demonstrate that C-X-C chemokine receptor type 7 (CXCR7), a seven-transmembrane G-protein-coupled chemokine receptor, is an AR-repressed gene and is upregulated after ADT. AR directly regulates CXCR7 using clustered regularly interspaced short palindromic repeats/CRISPR-associated protein 9 (CRISPR/Cas9) gene editing. Macrophage migration inhibitory factor (MIF) was identified as a ligand for CXCR7, which induces expression of cell-cycle genes through activating AKT signaling pathway. Previous studies have been focused on chemokine CXCL12 and its receptor CXCR4 in mediating metastasis of various cancer types, including prostate cancer. The critical roles of CXCL12/CXCR4 axis in the interaction between cancer cells and their microenvironment render it a promising therapeutic target in cancer treatment. The data suggest that the MIF/CXCR7/AKT pathway drives CRPC growth and metastasis independent of the CXCL12/CXCR4 axis. Furthermore, CXCR7 blockade in combination with anti-androgen enzalutamide inhibits CRPC tumor growth and potentially prevents metastasis. Notably, both MIF and CXCR7 are overexpressed in CRPC patient specimens and therefore are attractive therapeutic targets for these patients. IMPLICATIONS: This work suggests that CXCR7 plays more important roles than CXCR4 in CRPC progression; thus, targeting CXCR7 in combination with anti-androgen is a promising therapeutic approach for metastatic CRPC.
虽然雄激素剥夺疗法(ADT)是治疗转移性前列腺癌的有效方法,但不可避免地会发展为无法治愈的去势抵抗性前列腺癌(CRPC)。重要的是,雄激素受体(AR)在 ADT 后仍然是前列腺癌生长和进展的关键。其中一个潜在的分子机制是 ADT 后细胞周期和增殖相关的 AR 抑制基因的去抑制。在这里,数据表明,C-X-C 趋化因子受体 7(CXCR7),一种七跨膜 G 蛋白偶联趋化因子受体,是 AR 抑制基因,在 ADT 后上调。AR 通过使用簇状规则间隔的短回文重复序列/CRISPR 相关蛋白 9(CRISPR/Cas9)基因编辑直接调节 CXCR7。巨噬细胞移动抑制因子(MIF)被鉴定为 CXCR7 的配体,它通过激活 AKT 信号通路诱导细胞周期基因的表达。先前的研究集中在趋化因子 CXCL12 及其受体 CXCR4 介导各种癌症类型(包括前列腺癌)的转移。CXCL12/CXCR4 轴在癌细胞与其微环境相互作用中的关键作用使其成为癌症治疗中有前途的治疗靶点。数据表明,MIF/CXCR7/AKT 通路驱动 CRPC 的生长和转移,不依赖于 CXCL12/CXCR4 轴。此外,CXCR7 阻断联合抗雄激素恩扎鲁胺抑制 CRPC 肿瘤生长并可能防止转移。值得注意的是,MIF 和 CXCR7 在 CRPC 患者标本中均过度表达,因此是这些患者有吸引力的治疗靶点。意义:这项工作表明,CXCR7 在 CRPC 进展中的作用比 CXCR4 更为重要;因此,靶向 CXCR7 联合抗雄激素是治疗转移性 CRPC 的一种有前途的治疗方法。