Sandbakk Silvana B, Nauman Javaid, Lavie Carl J, Wisløff Ulrik, Stensvold Dorthe
K. G. Jebsen Center for Exercise in Medicine, Department of Circulation and Medical Imaging, Faculty of Medicine, Norwegian University of Science and Technology, Trondheim, Norway.
University of South Carolina, Columbia, SC.
Mayo Clin Proc Innov Qual Outcomes. 2017 May 12;1(1):67-77. doi: 10.1016/j.mayocpiqo.2017.05.001. eCollection 2017 Jul.
To investigate the independent and combined associations of fitness and fatness with cardiometabolic risk factors in older Norwegian women and men.
We conducted a cross-sectional study of 505 women and 417 men aged 70 to 77 years enrolled in the Generation 100 study in Norway. Fitness was assessed as peak oxygen uptake and fatness as high body mass index (BMI; ≥25 kg/m), waist circumference (WC) of 88 cm or greater for women and 102 cm or greater for men, and percent body fat (%BF) of 35% or greater and 25% or greater for women and men, respectively. High cardiometabolic risk was defined as the presence of 2 or more of the following risk factors: elevated triglyceride level, reduced high-density lipoprotein cholesterol concentration, elevated blood pressure, and elevated fasting glucose level or pharmacological treatment of these conditions.
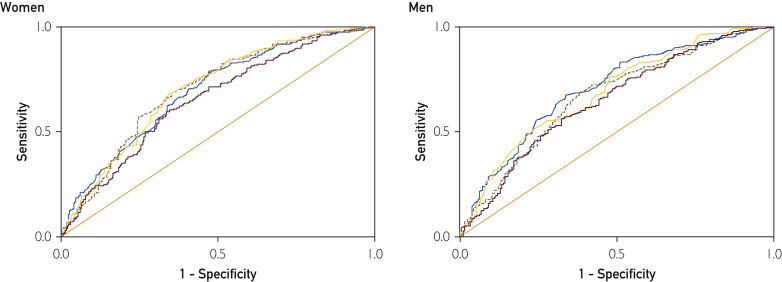
Receiver operating characteristic curve analyses identified fitness levels of less than 25.7 and less than 30.7 mL/kg per minute in women and men, respectively, as critical thresholds for having high cardiometabolic risk. Individuals with levels below these thresholds had an adjusted odds ratio of 2.77 (95% CI, 2.09-3.66) for having high cardiometabolic risk, while high BMI, WC, and %BF had odds ratios (95% CIs) of 3.58 (2.69-4.77), 3.06 (2.29-4.10), and 3.26 (2.47-4.30), respectively. In our combined analyses, being lean did not attenuate the cardiometabolic risk associated with low fitness, and combinations of low fitness and/or high BMI, WC, or %BF cumulatively increased cardiometabolic risk.
Low fitness and indication of fatness were independently and cumulatively associated with poor cardiometabolic health. Our results emphasize the importance of including both physical fitness and body fatness in the assessment of cardiometabolic risk and health promotion efforts in older adults.
探讨挪威老年女性和男性的身体适应性与肥胖程度与心血管代谢危险因素之间的独立关联及联合关联。
我们对挪威“百岁一代”研究中纳入的505名70至77岁女性和417名同龄男性进行了一项横断面研究。身体适应性通过峰值摄氧量进行评估,肥胖程度则依据高体重指数(BMI;≥25 kg/m²)、女性腰围88厘米及以上或男性腰围102厘米及以上,以及女性体脂百分比(%BF)35%及以上或男性体脂百分比25%及以上来判定。高心血管代谢风险被定义为存在以下两种或更多风险因素:甘油三酯水平升高、高密度脂蛋白胆固醇浓度降低、血压升高、空腹血糖水平升高或针对这些情况进行药物治疗。
受试者工作特征曲线分析确定,女性和男性每分钟每千克体重峰值摄氧量分别低于25.7和30.7毫升为具有高心血管代谢风险的临界阈值。低于这些阈值的个体具有高心血管代谢风险的校正比值比为2.77(第95百分位可信区间,2.09 - 3.66),而高BMI、腰围和%BF的比值比(第95百分位可信区间)分别为3.58(2.69 - 4.77)、3.06(2.29 - 4.10)和3.26(2.47 - 4.30)。在我们的联合分析中,体型偏瘦并未减轻与身体适应性差相关的心血管代谢风险,身体适应性差和/或高BMI、腰围或%BF的组合会累积增加心血管代谢风险。
身体适应性差和肥胖指征与不良心血管代谢健康状况独立且累积相关。我们的研究结果强调了在评估老年人心血管代谢风险和健康促进工作中纳入身体适应性和身体肥胖程度的重要性。