Tsukada Sachiyuki, Wakui Motohiro
Department of Orthopaedic Surgery, Nekoyama Miyao Hospital, Niigata, Niigata, Japan.
Department of Orthopaedic Surgery, Hokusuikai Kinen Hospital, Mito, Ibaraki, Japan.
JB JS Open Access. 2017 Apr 18;2(2):e0002. doi: 10.2106/JBJS.OA.17.00002. eCollection 2017 Jun 26.
A combined intravenous and intra-articular regimen is one of the most effective administration routes of tranexamic acid (TXA) to reduce perioperative blood loss in unilateral total knee arthroplasty. However, there have been few reports regarding use of the combined regimen for patients undergoing simultaneous bilateral total knee arthroplasty, in which blood-management strategy is more challenging.
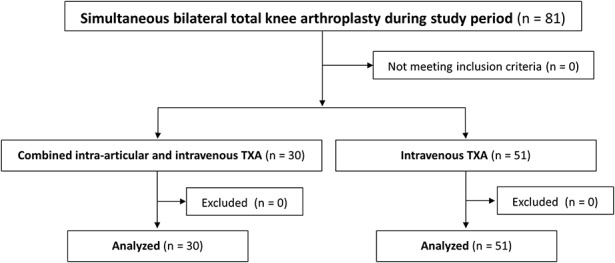
We compared perioperative blood loss in 30 consecutive patients undergoing simultaneous bilateral total knee arthroplasty who received both 1,000 mg of TXA intravenously and 1,000 mg of intra-articular TXA in each knee (combined TXA group) with that in a consecutive series of 51 patients who only received 1,000 mg of TXA intravenously (intravenous TXA group). Additional intravenous TXA was administered 6 hours after the initial administration in both groups. Except for the intraoperative TXA administration regimen, an identical perioperative blood-management strategy was applied to both groups; this consisted of transfusion of 800 or 400 mL of predeposited autologous blood except for patients with a preoperative hemoglobin level of <11.0 g/dL, who received 4 units of allogenic blood. All surgical procedures were performed with spinal anesthesia and without use of a pneumatic tourniquet. Perioperative blood loss was calculated using the blood volume and change in hemoglobin level from the preoperative measurement to postoperative day 3.
There was significantly less perioperative blood loss in the combined TXA group compared with the intravenous TXA group (mean and standard deviation, 1,201 ± 347 versus 1,638 ± 400 mL, respectively; mean difference, 437 mL; 95% confidence interval, 263 to 613 mL; p < 0.0001). No patient in the combined TXA group and 1 patient (2%) in the intravenous TXA group required additional allogenic blood transfusion. No thrombotic events occurred in either group.
In a nonrandomized comparison, combined intra-articular and intravenous TXA significantly reduced the calculated perioperative blood loss in simultaneous bilateral total knee arthroplasty compared with that found in patients treated only with intravenous TXA.
Therapeutic Level III. See Instructions for Authors for a complete description of levels of evidence.
静脉与关节内联合用药方案是氨甲环酸(TXA)减少单侧全膝关节置换术围手术期失血最有效的给药途径之一。然而,关于联合用药方案用于同期双侧全膝关节置换术患者的报道较少,而双侧手术的血液管理策略更具挑战性。
我们比较了30例连续接受同期双侧全膝关节置换术患者(联合TXA组)的围手术期失血量,这些患者每侧膝关节均静脉注射1000mg TXA并关节内注射1000mg TXA,与连续的51例仅静脉注射1000mg TXA的患者(静脉TXA组)的围手术期失血量。两组均在首次给药6小时后追加静脉注射TXA。除术中TXA给药方案外,两组采用相同的围手术期血液管理策略;具体为除术前血红蛋白水平<11.0g/dL的患者输注4单位异体血外,其余患者输注800或400mL预存自体血。所有手术均采用脊髓麻醉,不使用气压止血带。围手术期失血量通过术前至术后第3天的血容量和血红蛋白水平变化来计算。
联合TXA组的围手术期失血量显著少于静脉TXA组(均值和标准差分别为1201±347与1638±400mL;平均差值为437mL;95%置信区间为263至613mL;p<0.0001)。联合TXA组无患者需要额外输注异体血,静脉TXA组有1例患者(2%)需要额外输注异体血。两组均未发生血栓事件。
在非随机对照中,与仅接受静脉TXA治疗的患者相比,关节内与静脉联合使用TXA显著减少了同期双侧全膝关节置换术计算得出的围手术期失血量。
治疗性III级。有关证据级别的完整描述,请参阅作者须知。