Department of Global Health and Population, Harvard T.H. Chan School of Public Health, Harvard University, Boston, Massachusetts, United States of America.
Management and Development for Health, Dar es Salaam, Tanzania.
PLoS Med. 2018 Sep 19;15(9):e1002659. doi: 10.1371/journal.pmed.1002659. eCollection 2018 Sep.
With the increase in people living with HIV in sub-Saharan Africa and expanding eligibility criteria for antiretroviral therapy (ART), there is intense interest in the use of novel delivery models that allow understaffed health systems to successfully deal with an increasing demand for antiretroviral drugs (ARVs). This pragmatic randomized controlled trial in Dar es Salaam, Tanzania, evaluated a novel model of ARV community delivery: lay health workers (home-based carers [HBCs]) deliver ARVs to the homes of patients who are clinically stable on ART, while nurses and physicians deliver standard facility-based care for patients who are clinically unstable. Specifically, the trial aimed to assess whether the ARV community delivery model performed at least equally well in averting virological failure as the standard of care (facility-based care for all ART patients).
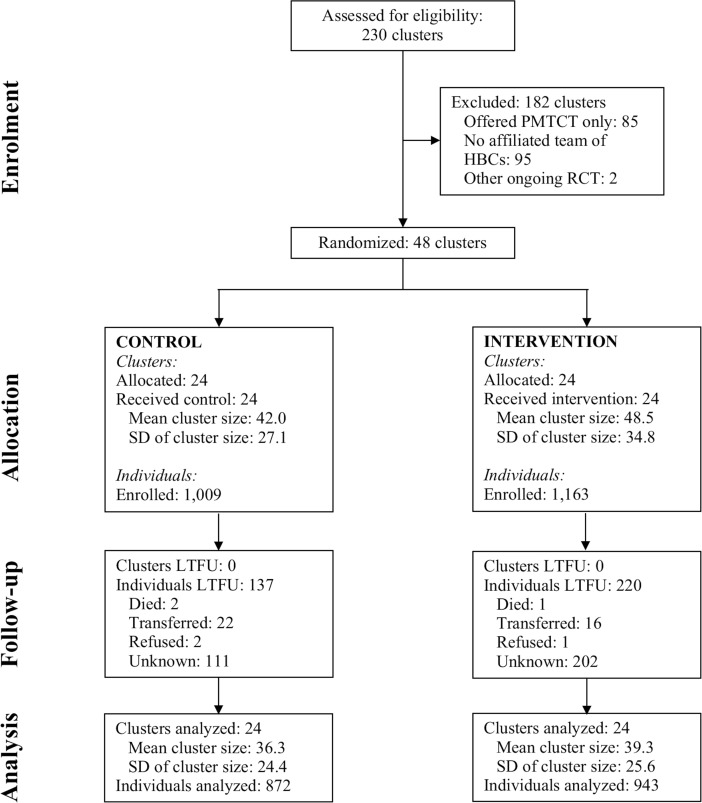
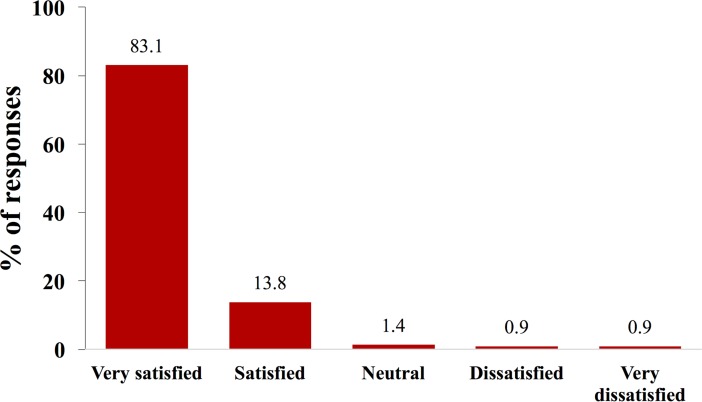
The study took place from March 1, 2016, to October 27, 2017. All (48) healthcare facilities in Dar es Salaam that provided ART and had an affiliated team of public-sector HBCs were randomized 1:1 to either (i) ARV community delivery (intervention) or (ii) the standard of care (control). Our prespecified primary endpoint was the proportion of adult non-pregnant ART patients with virological failure at the end of the study period. The prespecified margin of non-inferiority was a risk ratio (RR) of 1.45. The mean follow-up period was 326 days. We obtained intent-to-treat (ITT) RRs using a log-binomial model adjusting standard errors for clustering at the level of the healthcare facility. A total of 2,172 patients were enrolled at intervention (1,163 patients) and control (1,009 patients) facilities. Of the 1,163 patients in the intervention arm, 516 (44.4%) were both clinically stable on ART and opted to receive ARVs in their homes or at another meeting point of their choosing in the community. At the end of the study period, 10.9% (95/872) of patients in the control arm and 9.7% (91/943) in the intervention arm were failing virologically. The ITT RR for virological failure demonstrated non-inferiority of the ARV community delivery model (RR 0.89 [1-sided 95% CI 0.00-1.18]). We observed no significant difference between study arms in self-reported patient healthcare expenditures over the last 6 months before study exit. Of those who received ARVs in the community, 97.2% (95% CI 94.7%-98.7%) reported being either "satisfied" or "very satisfied" with the program. Other than loss to follow-up (18.9% in the intervention and 13.6% in the control arm), the main limitation of this trial was that substantial decongestion of healthcare facilities was not achieved, thus making the logic for our preregistered ITT approach (which includes those ineligible to receive ARVs at home in the intervention sample) less compelling.
In this study, an ARV community delivery model performed at least as well as the standard of care regarding the critical health indicator of virological failure. The intervention did not significantly reduce patient healthcare expenditures, but satisfaction with the program was high and it is likely to save patients time. Policy-makers should consider piloting, evaluating, and scaling more ambitious ARV community delivery programs that can reach higher proportions of ART patients.
ClinicalTrials.gov NCT02711293.
随着撒哈拉以南非洲地区艾滋病毒感染者人数的增加,以及抗逆转录病毒疗法(ART)的资格标准不断扩大,人们对新的药物输送模式产生了浓厚的兴趣,这些模式可以让人手不足的卫生系统成功应对日益增长的抗逆转录病毒药物(ARV)需求。坦桑尼亚达累斯萨拉姆的这项务实的随机对照试验评估了一种新的 ARV 社区输送模式:由经过培训的社区卫生工作者(家庭护理员)为正在接受 ART 治疗且临床稳定的患者提供 ARV 药物,而护士和医生则为临床不稳定的患者提供标准的医疗机构护理。具体来说,试验旨在评估 ARV 社区输送模式在预防病毒学失败方面是否至少与标准护理(所有接受 ART 治疗的患者均提供医疗机构护理)同样有效。
研究于 2016 年 3 月 1 日至 2017 年 10 月 27 日进行。达累斯萨拉姆的所有(48)家提供 ART 服务并拥有公共部门社区卫生工作者团队的医疗保健机构均按 1:1 的比例随机分为(i)ARV 社区输送(干预)或(ii)标准护理(对照)。我们预先指定的主要终点是研究结束时病毒学失败的成年非妊娠 ART 患者的比例。预先指定的非劣效性边缘是风险比(RR)为 1.45。平均随访时间为 326 天。我们使用对数二项式模型获得意向治疗(ITT)RR,该模型调整了医疗机构水平的聚类标准误差。共纳入 2172 名患者,分别在干预(1163 名患者)和对照(1009 名患者)设施中接受治疗。在干预组的 1163 名患者中,516 名(44.4%)患者在接受 ART 治疗时既临床稳定,又选择在家中或社区中的其他约定地点接受 ARV 药物。研究结束时,对照组的 10.9%(95/872)和干预组的 9.7%(91/943)的患者病毒学失败。ITT 分析显示,ARV 社区输送模式不劣于标准护理(RR 0.89 [单侧 95%CI 0.00-1.18])。我们在研究退出前的最后 6 个月内,未观察到研究组之间在患者医疗保健支出方面有显著差异。在接受社区 ARV 治疗的患者中,97.2%(95%CI 94.7%-98.7%)报告对该项目“满意”或“非常满意”。除了失访(干预组 18.9%,对照组 13.6%)之外,本试验的主要局限性是医疗保健机构的拥堵状况并未得到显著缓解,因此我们预先注册的 ITT 方法(包括那些不符合在家接受 ARV 治疗条件的患者)的逻辑依据不太充分。
在这项研究中,ARV 社区输送模式在病毒学失败这一关键健康指标方面的表现至少与标准护理相当。该干预措施并未显著降低患者的医疗保健支出,但患者对该项目的满意度很高,并且可能为患者节省时间。政策制定者应考虑试点、评估和推广更具雄心的 ARV 社区输送项目,以覆盖更多的接受 ART 治疗的患者。
ClinicalTrials.gov NCT02711293。