Center for Health and the Social Sciences, University of Chicago, 5841 S. Maryland Avenue, MC 1005, Suite M200, Chicago, IL, USA.
School of Public Health, University of the Western Cape, Robert Sobukwe Road, Bellville, 7535, Republic of South Africa.
Int J Equity Health. 2018 Sep 24;17(1):142. doi: 10.1186/s12939-018-0824-y.
Medical specialization is a key feature of biomedicine, and is a growing, but weakly understood aspect of health systems in many low- and middle-income countries (LMICs), including India. Emergency medicine is an example of a medical specialty that has been promoted in India by several high-income country stakeholders, including the Indian diaspora, through transnational and institutional partnerships. Despite the rapid evolution of emergency medicine in comparison to other specialties, this specialty has seen fragmentation in the stakeholder network and divergent training and policy objectives. Few empirical studies have examined the influence of stakeholders from high-income countries broadly, or of diasporas specifically, in transferring knowledge of medical specialization to LMICs. Using the concepts of socialization and legitimation, our goal is to examine the transfer of medical knowledge from high-income countries to LMICs through domestic, diasporic and foreign stakeholders, and the perceived impact of this knowledge on shaping health priorities in India.
This analysis was conducted as part of a broader study on the development of emergency medicine in India. We designed a qualitative case study focused on the early 1990s until 2015, analyzing data from in-depth interviewing (n = 87), document review (n = 248), and non-participant observation of conferences and meetings (n = 6).
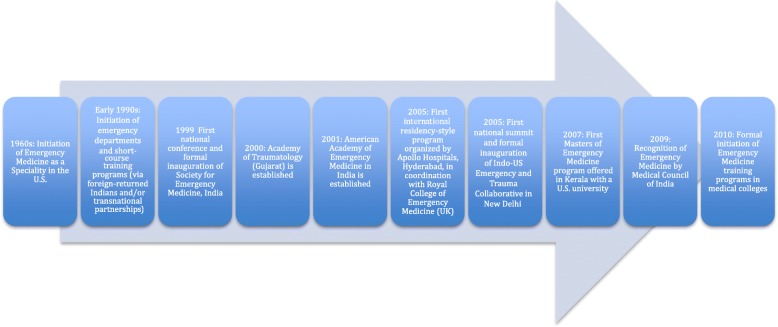
From the early 1990s, domestic stakeholders with exposure to emergency medicine in high-income countries began to establish Emergency Departments and initiate specialist training in the field. Their efforts were amplified by the active legitimation of emergency medicine by diasporic and foreign stakeholders, who formed transnational partnerships with domestic stakeholders and organized conferences, training programs and other activities to promote the field in India. However, despite a broad commitment to expanding specialist training, the network of domestic, diasporic and foreign stakeholders was highly fragmented, resulting in myriad unstandardized postgraduate training programs and duplicative policy agendas. Further, the focus in this time period was largely on training specialists, resulting in more emphasis on a medicalized, tertiary-level form of care.
This analysis reveals the complexities of the roles and dynamics of domestic, diasporic and foreign stakeholders in the evolution of emergency medicine in India. More research and critical analyses are required to explore the transfer of medical knowledge, such as other medical specialties, models of clinical care, and medical technologies, from high-income countries to India.
医学专业化是生物医学的一个重要特征,也是许多低收入和中等收入国家(LMICs),包括印度,卫生系统日益发展但理解薄弱的一个方面。急诊医学就是一个通过跨国和机构伙伴关系,由包括印度侨民在内的几个高收入国家利益攸关方在印度推广的医学专业范例。尽管与其他专业相比,急诊医学的发展迅速,但该专业的利益攸关者网络已经出现分裂,培训和政策目标也出现分歧。很少有实证研究从广义上考察高收入国家的利益攸关者,或专门考察侨民,考察他们将医学专业化知识转移到 LMICs 的情况。利用社会化和合法化的概念,我们的目标是研究通过国内、侨民和外国利益攸关者从高收入国家向 LMICs 转移医学知识,以及这种知识对塑造印度卫生重点的感知影响。
本分析是印度急诊医学发展的更广泛研究的一部分。我们设计了一项定性案例研究,重点关注 20 世纪 90 年代初至 2015 年,对深入访谈(n=87)、文件审查(n=248)和非参与式会议和会议观察(n=6)进行分析。
从 20 世纪 90 年代初开始,接触过高收入国家急诊医学的国内利益攸关方开始建立急诊部并开始在该领域进行专业培训。侨民和外国利益攸关方积极使急诊医学合法化,他们与国内利益攸关方建立跨国伙伴关系,并组织会议、培训计划和其他活动,以促进印度的这一领域,这扩大了他们的努力。然而,尽管有广泛的扩大专科培训的承诺,但国内、侨民和外国利益攸关者的网络高度分散,导致无数非标准化的研究生培训计划和重复的政策议程。此外,在这一时期,重点主要是培训专家,因此更注重一种医疗化的、三级护理形式的护理。
本分析揭示了国内、侨民和外国利益攸关方在印度急诊医学发展中的角色和动态的复杂性。需要进行更多的研究和批判性分析,以探讨从高收入国家向印度转移医学知识,如其他医学专业、临床护理模式和医疗技术。