McCarter Allison R, Timm Paul C, Shepard Paul W, Sandness David J, Luu Thao, McCarter Stuart J, Dueffert Lucas, Dresow Max, Feemster John C, Cascino Gregory D, So Elson L, Worrell Gregory A, Britton Jeffrey W, Sherif Akil, Jaliparthy Keerthi, Chahal Anwar A, Somers Virend K, St Louis Erik K
Mayo Center for Sleep Medicine, Mayo Clinic and Foundation, Rochester, Minnesota.
Department of Medicine, Mayo Clinic and Foundation, Rochester, Minnesota.
Epilepsia. 2018 Oct;59(10):1973-1981. doi: 10.1111/epi.14548. Epub 2018 Sep 24.
We aimed to determine the frequency of probable obstructive sleep apnea (pOSA) in refractory epilepsy monitoring unit inpatients and clinical features associated with pOSA, including risk for sudden unexpected death in epilepsy (SUDEP).
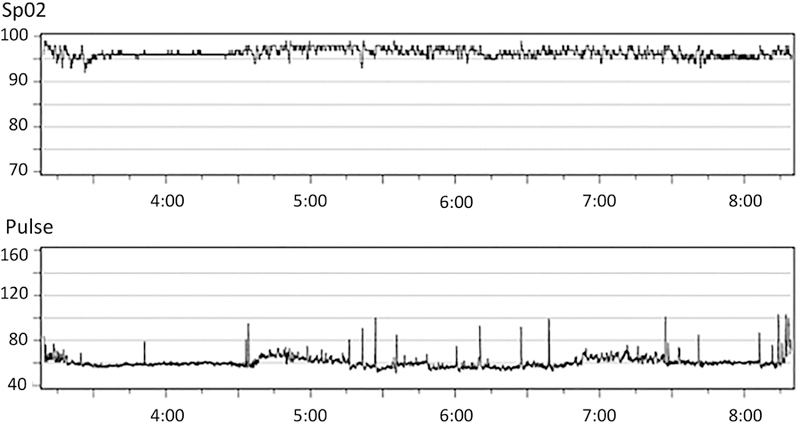
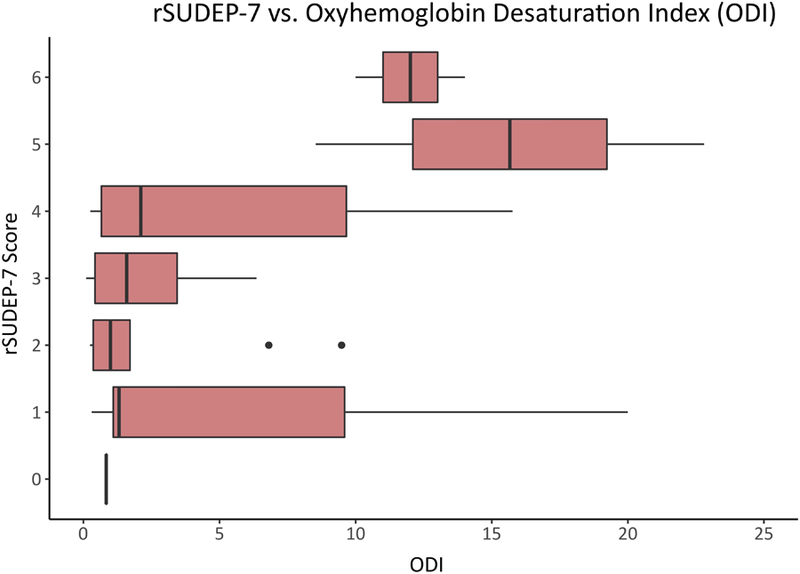
We prospectively recruited 49 consecutive adult patients admitted to the Mayo Clinic Epilepsy Monitoring Unit with focal, generalized, or unclassified epilepsy syndromes. pOSA was identified using oximetric oxyhemoglobin desaturation index (ODI) and the Sleep Apnea-Sleep Disorders Questionnaire (SA-SDQ) and STOP-BAG screening tools. Revised SUDEP Risk Inventory (rSUDEP-7) scores were calculated, and epilepsy patients with and without pOSA were compared with Wilcoxon signed-rank tests. Correlation and regression analyses were utilized to determine relationships between pOSA and rSUDEP-7 scores.
Thirty-five percent of patients had pOSA, with a mean ODI of 11.3 ± 5.1/h (range = 5.1-22.8). Patients with pOSA were older and heavier, and more frequently had a focal epilepsy syndrome and longer epilepsy duration, with higher SA-SDQ and STOP-BAG scores (all P < 0.05). Median rSUDEP-7 score was 3 ± 1.4 (range = 0-6). Higher rSUDEP-7 scores were positively correlated with higher ODI (P = 0.036). rSUDEP-7 score ≥ 5 was associated with pOSA by ODI, SA-SDQ, and STOP-BAG questionnaire criteria (P < 0.05).
Our pilot study identified a high frequency of pOSA in refractory epilepsy monitoring patients, finding that pOSA patients were older and heavier, with higher screening symptoms for sleep apnea and more frequent focal seizures with a longer epilepsy duration. We also found a possible association between OSA and SUDEP risk. Identification and treatment of OSA in patients with epilepsy could conceivably provide a novel approach toward preventing the risk of SUDEP. Future studies with polysomnography are needed to confirm predictive features for OSA in epilepsy populations, and to determine whether OSA is associated with SUDEP risk.
我们旨在确定难治性癫痫监测单元住院患者中可能的阻塞性睡眠呼吸暂停(pOSA)的发生率以及与pOSA相关的临床特征,包括癫痫猝死(SUDEP)风险。
我们前瞻性招募了49例连续入住梅奥诊所癫痫监测单元的成年患者,这些患者患有局灶性、全身性或未分类的癫痫综合征。使用血氧饱和度氧合血红蛋白去饱和指数(ODI)以及睡眠呼吸暂停-睡眠障碍问卷(SA-SDQ)和STOP-BAG筛查工具来识别pOSA。计算修订后的SUDEP风险量表(rSUDEP-7)得分,并使用Wilcoxon符号秩检验比较有无pOSA的癫痫患者。利用相关性和回归分析来确定pOSA与rSUDEP-7得分之间的关系。
35%的患者存在pOSA,平均ODI为11.3±5.1次/小时(范围=5.1-22.8)。有pOSA的患者年龄更大、体重更重,更频繁地患有局灶性癫痫综合征且癫痫病程更长,SA-SDQ和STOP-BAG得分更高(所有P<0.05)。rSUDEP-7得分中位数为3±1.4(范围=0-6)。较高的rSUDEP-7得分与较高的ODI呈正相关(P=0.036)。根据ODI、SA-SDQ和STOP-BAG问卷标准,rSUDEP-7得分≥5与pOSA相关(P<0.05)。
我们的初步研究发现难治性癫痫监测患者中pOSA的发生率很高,发现pOSA患者年龄更大、体重更重,睡眠呼吸暂停筛查症状更严重,局灶性发作更频繁且癫痫病程更长。我们还发现OSA与SUDEP风险之间可能存在关联。识别和治疗癫痫患者的OSA可能为预防SUDEP风险提供一种新方法。未来需要进行多导睡眠图研究,以确认癫痫人群中OSA的预测特征,并确定OSA是否与SUDEP风险相关。