Cutler Eli, Karaca Zeynal, Henke Rachel, Head Michael, Wong Herbert S
1 IBM Watson Health, Cambridge, MA, USA.
2 U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality, Rockville, MD, USA.
Inquiry. 2018 Jan-Dec;55:46958018800092. doi: 10.1177/0046958018800092.
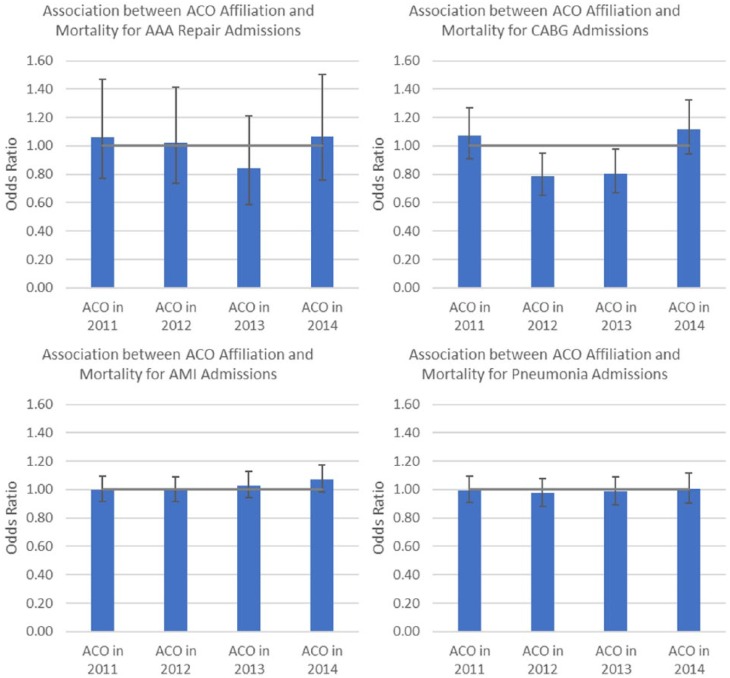
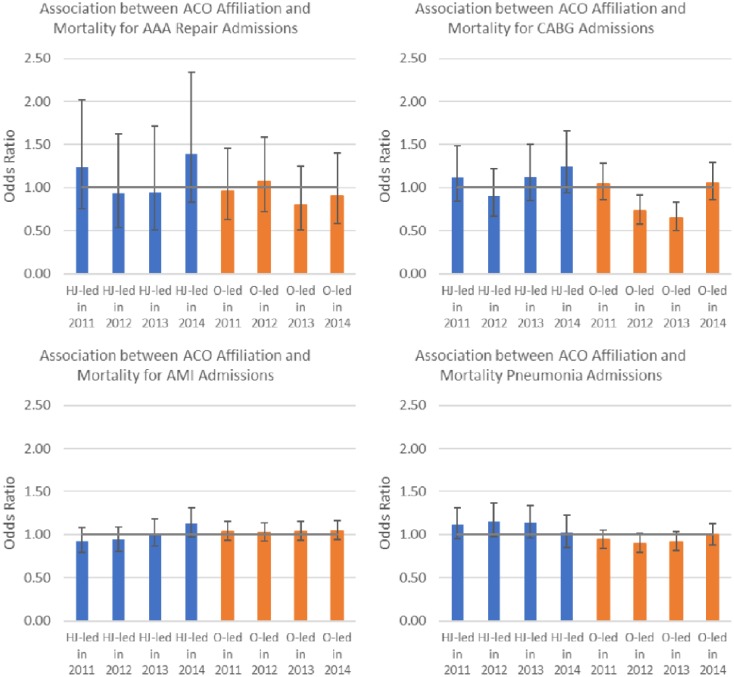
Studies have linked Accountable Care Organizations (ACOs) to improved primary care, but there is little research on how ACOs affect care in other settings. We examined whether Medicare ACOs have improved hospital quality of care, specifically focusing on preventable inpatient mortality. We used 2008-2014 Healthcare Cost and Utilization Project hospital discharge data from 34 states' Medicare ACO and non-ACO hospitals in conjunction with data from the American Hospital Association Annual Survey and the Survey of Care Systems and Payment. We estimated discharge-level logistic regression models that measured the relationship between ACO affiliation and mortality following admissions for acute myocardial infarction, abdominal aortic aneurysm (AAA) repair, coronary artery bypass grafting, and pneumonia, controlling for patient demographic mix, hospital, and year. Our results suggest that, on average, Medicare ACO hospitals are not associated with improved mortality rates for the studied IQI conditions. Stakeholders may potentially consider providing ACOs with incentives or designing new programs for ACOs to target inpatient mortality reductions.
研究已将责任医疗组织(ACO)与改善初级医疗联系起来,但关于ACO如何影响其他医疗环境下的医疗服务,相关研究甚少。我们研究了医疗保险ACO是否提高了医院的医疗质量,特别关注可预防的住院死亡率。我们使用了2008 - 2014年医疗成本和利用项目中来自34个州医疗保险ACO医院和非ACO医院的出院数据,并结合了美国医院协会年度调查以及医疗系统与支付调查的数据。我们估计了出院水平的逻辑回归模型,该模型衡量了ACO附属关系与急性心肌梗死、腹主动脉瘤(AAA)修复、冠状动脉搭桥术和肺炎入院后死亡率之间的关系,同时控制了患者人口统计学构成、医院和年份等因素。我们的结果表明,平均而言,医疗保险ACO医院与所研究的质量指标改进(IQI)状况下的死亡率改善并无关联。利益相关者可能会考虑为ACO提供激励措施或为ACO设计新的项目,以降低住院死亡率。