Development Research Group, The World Bank, Washington, District of Columbia, United States of America.
University of California at Berkeley, Berkeley, California, United States of America.
PLoS Med. 2018 Sep 25;15(9):e1002653. doi: 10.1371/journal.pmed.1002653. eCollection 2018 Sep.
India has the highest burden of tuberculosis (TB). Although most patients with TB in India seek care from the private sector, there is limited evidence on quality of TB care or its correlates. Following our validation study on the standardized patient (SP) method for TB, we utilized SPs to examine quality of adult TB care among health providers with different qualifications in 2 Indian cities.
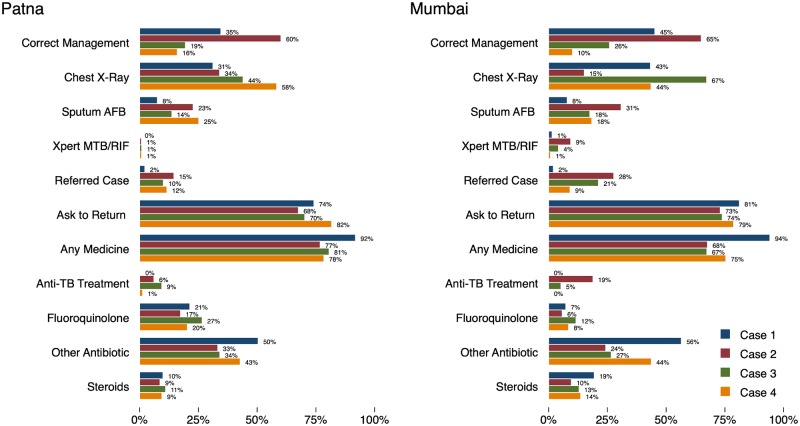
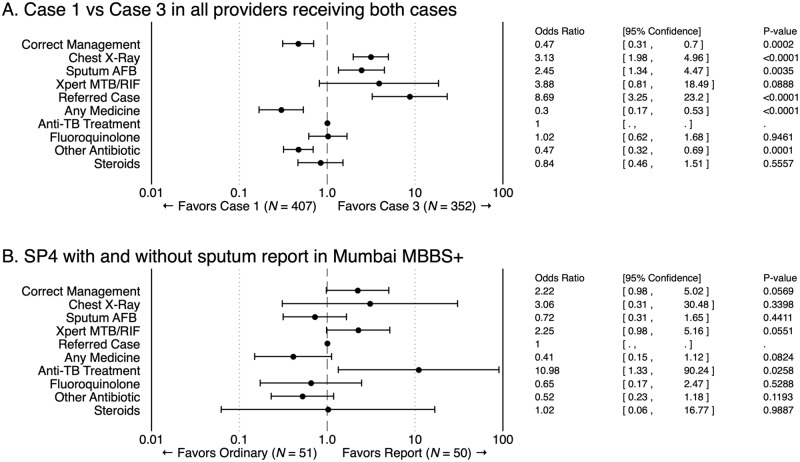
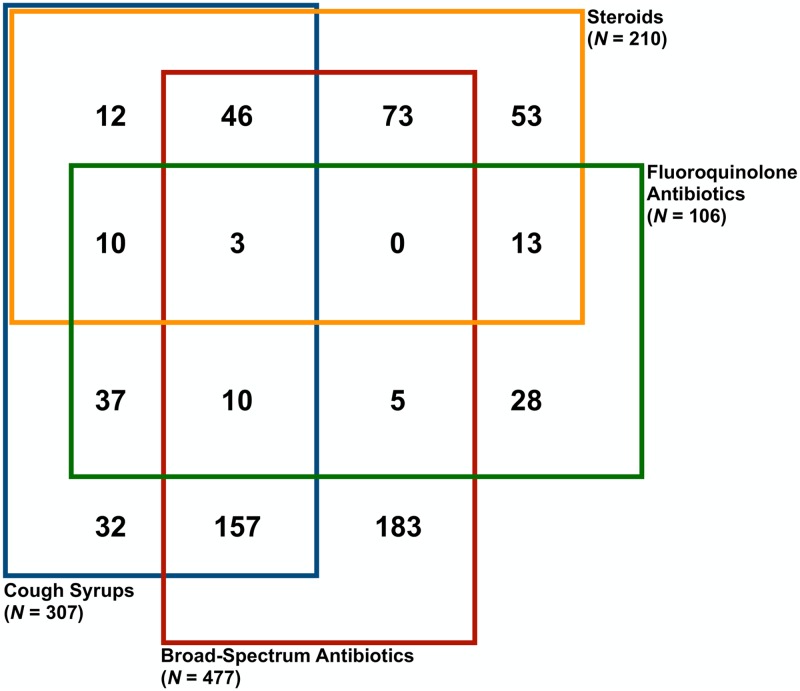
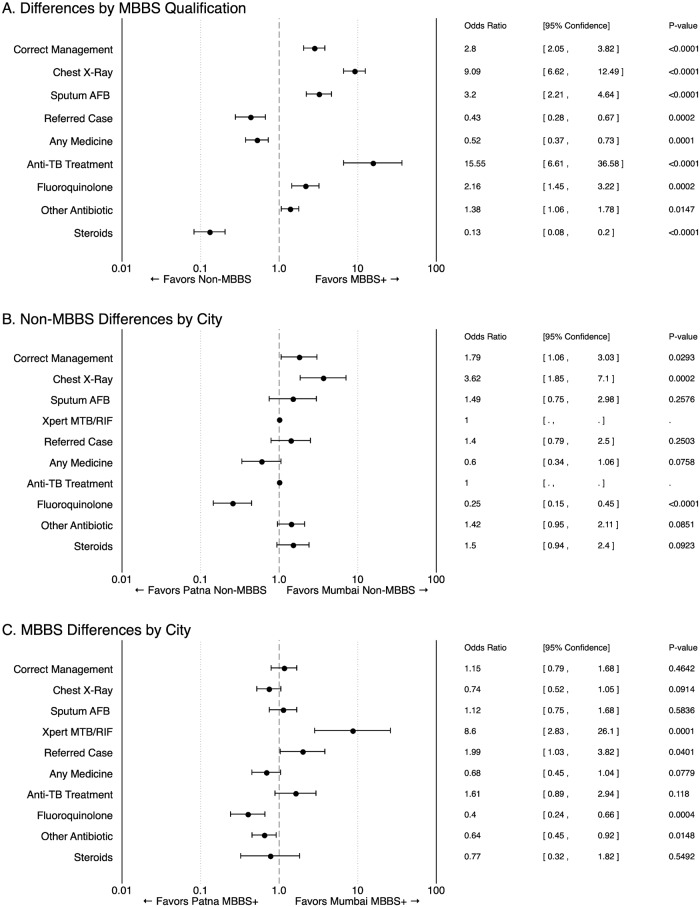
During 2014-2017, pilot programs engaged the private health sector to improve TB management in Mumbai and Patna. Nested within these projects, to obtain representative, baseline measures of quality of TB care at the city level, we recruited 24 adults to be SPs. They were trained to portray 4 TB "case scenarios" representing various stages of disease and diagnostic progression. Between November 2014 and August 2015, the SPs visited representatively sampled private providers stratified by qualification: (1) allopathic providers with Bachelor of Medicine, Bachelor of Surgery (MBBS) degrees or higher and (2) non-MBBS providers with alternative medicine, minimal, or no qualifications. Our main outcome was case-specific correct management benchmarked against the Standards for TB Care in India (STCI). Using ANOVA, we assessed variation in correct management and quality outcomes across (a) cities, (b) qualifications, and (c) case scenarios. Additionally, 2 micro-experiments identified sources of variation: first, quality in the presence of diagnostic test results certainty and second, provider consistency for different patients presenting the same case. A total of 2,652 SP-provider interactions across 1,203 health facilities were analyzed. Based on our sampling strategy and after removing 50 micro-experiment interactions, 2,602 interactions were weighted for city-representative interpretation. After weighting, the 473 Patna providers receiving SPs represent 3,179 eligible providers in Patna; in Mumbai, the 730 providers represent 7,115 eligible providers. Correct management was observed in 959 out of 2,602 interactions (37%; 35% weighted; 95% CI 32%-37%), primarily from referrals and ordering chest X-rays (CXRs). Unnecessary medicines were given to nearly all SPs, and antibiotic use was common. Anti-TB drugs were prescribed in 118 interactions (4.5%; 5% weighted), of which 45 were given in the case in which such treatment is considered correct management. MBBS and more qualified providers had higher odds of correctly managing cases than non-MBBS providers (odds ratio [OR] 2.80; 95% CI 2.05-3.82; p < 0.0001). Mumbai non-MBBS providers had higher odds of correct management than non-MBBS in Patna (OR 1.79; 95% CI 1.06-3.03), and MBBS providers' quality of care did not vary between cities (OR 1.15; 95% CI 0.79-1.68; p = 0.4642). In the micro-experiments, improving diagnostic certainty had a positive effect on correct management but not across all quality dimensions. Also, providers delivered idiosyncratically consistent care, repeating all observed actions, including mistakes, approximately 75% of the time. The SP method has limitations: it cannot account for patient mix or care-management practices reflecting more than one patient-provider interaction.
Quality of TB care is suboptimal and variable in urban India's private health sector. Addressing this is critical for India's plans to end TB by 2025. For the first time, we have rich measures on representative levels of care quality from 2 cities, which can inform private-sector TB interventions and quality-improvement efforts.
印度是结核病(TB)负担最重的国家。尽管印度大多数结核病患者都在私营部门寻求治疗,但有关结核病护理质量或其相关因素的证据有限。在对标准化患者(SP)方法进行验证研究之后,我们利用 SP 检查了印度两个城市不同资质的卫生提供者中成人结核病护理的质量。
2014-2017 年,试点项目利用私营部门来改善孟买和巴特那的结核病管理。作为这些项目的一部分,为了在城市层面获得结核病护理质量的代表性、基线测量值,我们招募了 24 名成年人作为 SP。他们接受了培训,以扮演 4 个结核病“病例场景”,代表疾病和诊断进展的各个阶段。2014 年 11 月至 2015 年 8 月,SP 按资质分层(1)具有医学学士、外科学士学位或更高学历的全科学历提供者和(2)具有替代医学、最低学历或无学历的非 MBBS 提供者,对代表性抽样的私人提供者进行了访问。我们的主要结果是针对印度结核病护理标准(STCI)的特定病例的正确管理基准。使用方差分析,我们评估了(a)城市、(b)资质和(c)病例场景之间正确管理和质量结果的差异。此外,两项微观实验确定了变异的来源:首先,在诊断测试结果确定的情况下的质量,其次,对于呈现相同病例的不同患者的提供者一致性。对 1203 个卫生机构的 2652 次 SP-提供者互动进行了分析。根据我们的抽样策略,并在去除 50 次微观实验互动后,对 2602 次互动进行了加权,以进行城市代表性解释。加权后,在巴特那接受 SP 的 473 名提供者代表巴特那的 3179 名合格提供者;在孟买,730 名提供者代表 7115 名合格提供者。在 2602 次互动中,有 959 次(37%;5%加权;95%CI 32%-37%)观察到正确管理,主要来自转诊和胸部 X 光检查(CXR)。几乎所有的 SP 都接受了不必要的药物治疗,抗生素的使用也很常见。在 118 次互动中(4.5%;5%加权)开具了抗结核病药物,其中 45 次开具了这种治疗被认为是正确管理的病例。MBBS 和更合格的提供者比非 MBBS 提供者更有可能正确管理病例(比值比[OR]2.80;95%CI 2.05-3.82;p<0.0001)。与巴特那的非 MBBS 提供者相比,孟买的非 MBBS 提供者更有可能正确管理病例(OR 1.79;95%CI 1.06-3.03),而 MBBS 提供者的护理质量在城市之间没有差异(OR 1.15;95%CI 0.79-1.68;p=0.4642)。在微观实验中,提高诊断确定性对正确管理有积极影响,但不是对所有质量维度都有影响。此外,提供者以独特的一致方式提供护理,大约 75%的时间重复所有观察到的动作,包括错误。SP 方法有其局限性:它不能说明患者的构成或反映不止一次患者-提供者互动的护理管理实践。
印度私营部门的结核病护理质量不尽如人意且存在差异。解决这一问题对于印度到 2025 年结束结核病的计划至关重要。我们首次从两个城市获得了有关代表性护理质量水平的丰富措施,这些措施可以为私营部门结核病干预措施和质量改进工作提供信息。