Development Research Group, The World Bank, Washington, DC, USA.
Development Research Group, The World Bank, Washington, DC, USA; University of California at Berkeley, Berkeley, CA, USA.
Lancet Glob Health. 2019 May;7(5):e633-e643. doi: 10.1016/S2214-109X(19)30031-2. Epub 2019 Mar 27.
In India, men are more likely than women to have active tuberculosis but are less likely to be diagnosed and notified to national tuberculosis programmes. We used data from standardised patient visits to assess whether these gender differences occur because of provider practice.
We sent standardised patients (people recruited from local populations and trained to portray a scripted medical condition to health-care providers) to present four tuberculosis case scenarios to private health-care providers in the cities of Mumbai and Patna. Sampling and weighting allowed for city representative interpretation. Because standardised patients were assigned to providers by a field team blinded to this study, we did balance and placebo regression tests to confirm standardised patients were assigned by gender as good as randomly. Then, by use of linear and logistic regression, we assessed correct case management, our primary outcome, and other dimensions of care by standardised patient gender.
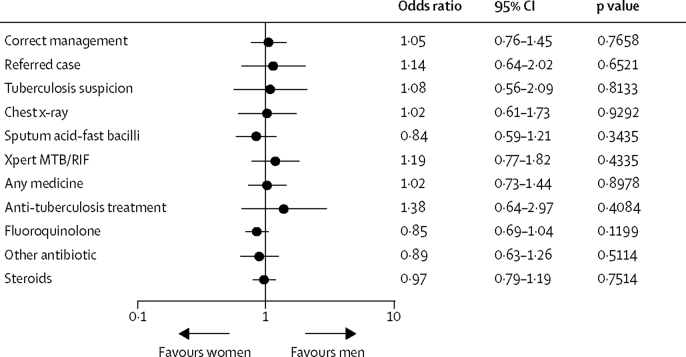
Between Nov 21, 2014, and Aug 21, 2015, 2602 clinical interactions at 1203 private facilities were completed by 24 standardised patients (16 men, eight women). We found standardised patients were assigned to providers as good as randomly. We found no differences in correct management by patient gender (odds ratio 1·05; 95% CI 0·76-1·45; p=0·77) and no differences across gender within any case scenario, setting, provider gender, or provider qualification.
Systematic differences in quality of care are unlikely to be a cause of the observed under-representation of men in tuberculosis notifications in the private sector in urban India.
Grand Challenges Canada, Bill & Melinda Gates Foundation, World Bank Knowledge for Change Program.
在印度,男性比女性更有可能患有活动性肺结核,但被诊断出来并通知国家结核病规划的可能性较小。我们使用标准化患者就诊的数据来评估这些性别差异是否是由于提供者的做法造成的。
我们派遣标准化患者(从当地人群中招募并接受培训,以向医疗保健提供者描绘既定医疗状况的人员)向孟买和巴特那市的私营医疗机构的医生展示了四个肺结核病例场景。抽样和加权允许对城市进行有代表性的解释。由于标准化患者是由对该研究不知情的现场小组分配给提供者的,因此我们进行了平衡和安慰剂回归测试,以确认标准化患者的分配是随机的。然后,我们使用线性和逻辑回归评估了正确的病例管理(我们的主要结果)和标准化患者性别的其他护理维度。
2014 年 11 月 21 日至 2015 年 8 月 21 日,24 名标准化患者在 1203 家私营医疗机构完成了 2602 次临床互动(16 名男性,8 名女性)。我们发现标准化患者的分配与随机分配一样好。我们没有发现患者性别对正确管理的影响存在差异(比值比 1.05;95%CI 0.76-1.45;p=0.77),在任何病例场景、设置、提供者性别或提供者资质中,也没有发现性别之间的差异。
在印度城市私营部门中,由于系统的护理质量差异,男性在结核病通知中代表性不足的情况不太可能是原因。
加拿大大挑战、比尔和梅琳达盖茨基金会、世界银行知识换变革计划。