Tseng Li-Jung, Yu Hsi-Yu, Wang Chih-Hsien, Chi Nai-Hsin, Huang Shu-Chien, Chou Heng-Wen, Shih Hsin-Chin, Chou Nai-Kuan, Chen Yih-Sharng
Institute of Emergency and Critical Care Medicine, National Yang-Ming University, Taipei 10644, Taiwan.
Department of Surgery, National Taiwan University Hospital, and College of Medicine, National Taiwan University, No.7, Chung-Shan South Road, Taipei 10002, Taiwan.
J Clin Med. 2018 Sep 29;7(10):313. doi: 10.3390/jcm7100313.
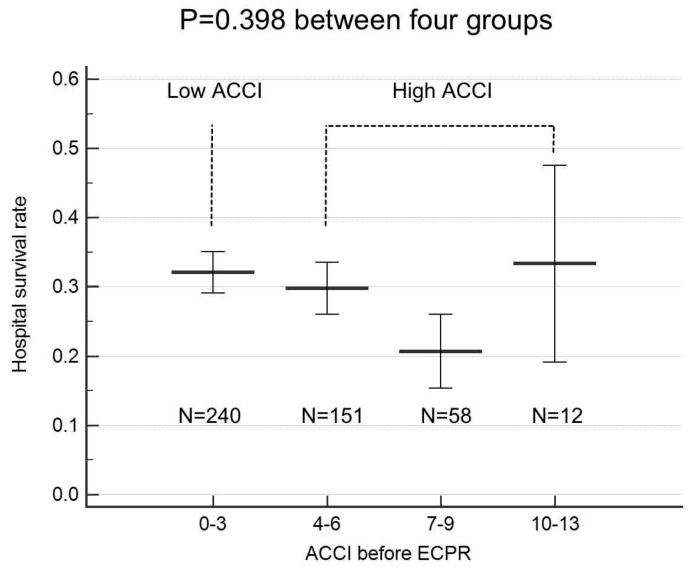
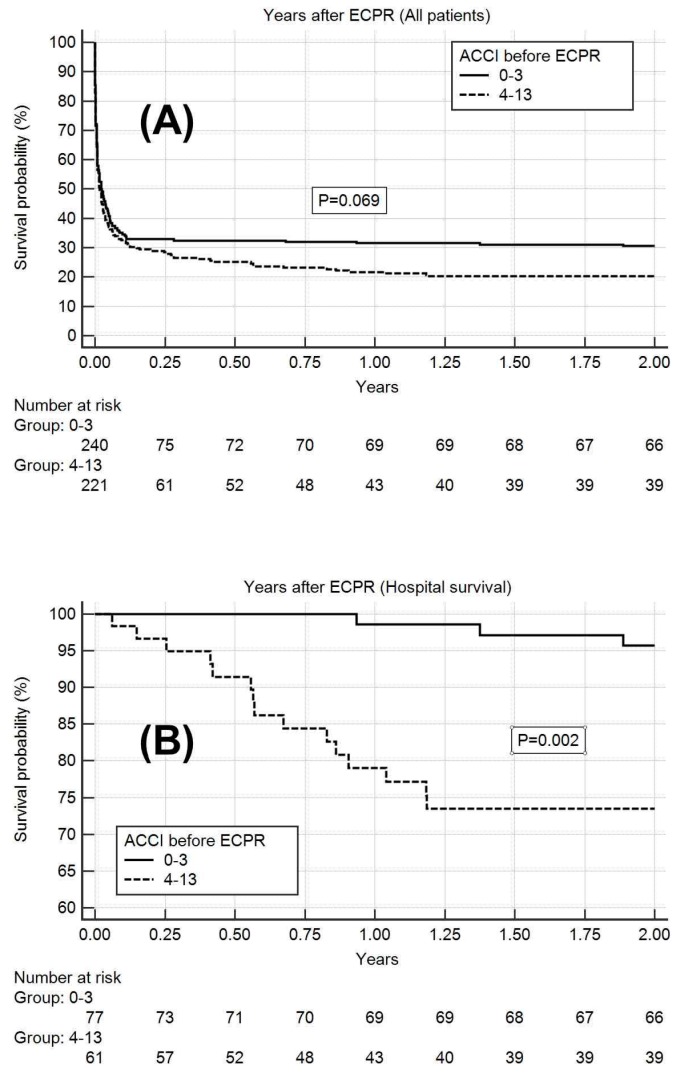
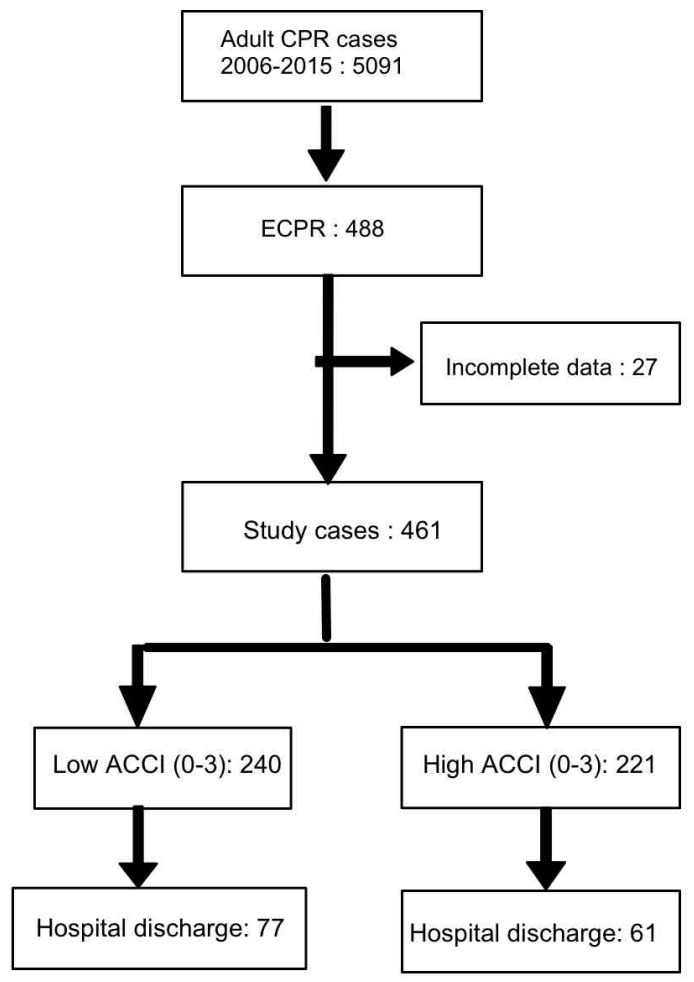
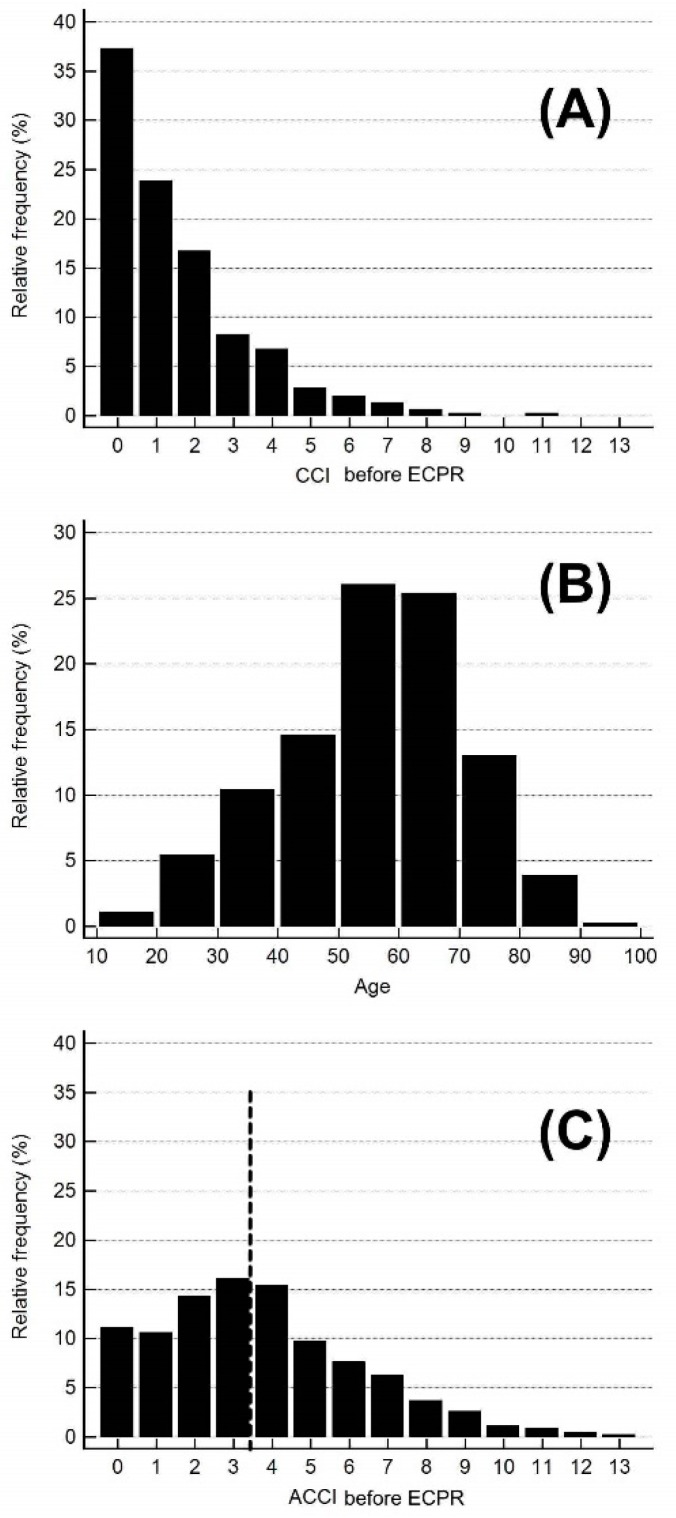
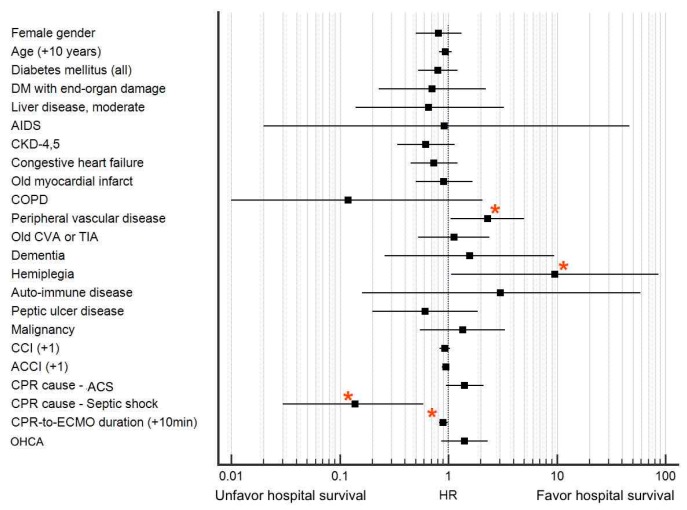
Extracorporeal cardiopulmonary resuscitation (ECPR) has gradually come to be regarded as an effective therapy, but the hospital mortality rate after ECPR is still high and unpredictable. The present study tested whether age-adjusted Charlson comorbidity index (ACCI) can be used as an objective selection criterion to ensure the most efficient utilization of medical resources. Adult patients (age ≥ 18 years) receiving ECPR at our institution between 2006 and 2015 were included. Data regarding ECPR events and ACCI characteristics were collected immediately after the extracorporeal membrane oxygenation (ECMO) setup. Adverse events during hospitalization were also prospectively collected. The primary endpoint was survival to hospital discharge. The second endpoint was the short-term (2-year) follow-up outcome. A total of 461 patients included in the study were grouped into low ACCI (ACCI 0⁻3) (240, 52.1%) and high ACCI (ACCI 4⁻13) (221, 47.9%) groups. The median ACCI was 2 (interquartile range (IQR): 1⁻3) and 5 (IQR: 4⁻7) for the low and high ACCI groups, respectively. Cardiopulmonary resuscitation (CPR)-to-ECMO duration was comparable between the groups (42.1 ± 25.6 and 41.3 ± 20.7 min in the low and high ACCI groups, respectively; = 0.754). Regarding the hospital survival rate, 256 patients (55.5%) died on ECMO support. A total of 205 patients (44.5%) were successfully weaned off ECMO, but only 138 patients (29.9%) survived to hospital discharge (32.1% and 27.6% in low and high ACCI group, = 0.291). Multivariate logistic regression analysis revealed CPR duration before ECMO run (CPR-to-ECMO duration) and a CPR cause of septic shock to be significant risk factors for hospital survival after ECPR ( = 0.043 and 0.014, respectively), whereas age and ACCI were not ( = 0.334 and 0.164, respectively). The 2-year survival rate after hospital discharge for the 138 hospital survivors was 96% and 74% in the low and high ACCI groups, respectively ( = 0.002). High ACCI before ECPR does not predict a poor outcome of hospital survival. Therefore, ECPR should not be rejected solely due to high ACCI. However, high ACCI in hospital survivors is associated with a higher 2-year mortality rate than low ACCI, and patients with high ACCI should be closely followed up.
体外心肺复苏(ECPR)已逐渐被视为一种有效的治疗方法,但ECPR后的医院死亡率仍然很高且难以预测。本研究测试了年龄调整后的查尔森合并症指数(ACCI)是否可作为一种客观的选择标准,以确保医疗资源的最有效利用。纳入了2006年至2015年期间在我们机构接受ECPR的成年患者(年龄≥18岁)。在体外膜肺氧合(ECMO)设置后立即收集有关ECPR事件和ACCI特征的数据。还前瞻性收集了住院期间的不良事件。主要终点是存活至出院。第二个终点是短期(2年)随访结果。该研究共纳入的461例患者被分为低ACCI(ACCI 0⁻3)组(240例,52.1%)和高ACCI(ACCI 4⁻13)组(221例,47.9%)。低ACCI组和高ACCI组的ACCI中位数分别为2(四分位间距(IQR):1⁻3)和5(IQR:4⁻7)。两组之间的心肺复苏(CPR)至ECMO持续时间相当(低ACCI组和高ACCI组分别为42.1±25.6分钟和41.3±20.7分钟;P = 0.754)。关于医院生存率,256例患者(55.5%)在ECMO支持下死亡。共有205例患者(44.5%)成功撤离ECMO,但只有138例患者(29.9%)存活至出院(低ACCI组和高ACCI组分别为32.1%和27.6%,P = 0.291)。多因素逻辑回归分析显示,ECMO运行前的CPR持续时间(CPR至ECMO持续时间)和感染性休克的CPR病因是ECPR后医院生存的重要危险因素(分别为P = 0.043和0.014),而年龄和ACCI则不是(分别为P = 0.334和0.164)。138例医院幸存者出院后的2年生存率在低ACCI组和高ACCI组分别为96%和74%(P = 0.002)。ECPR前高ACCI并不能预测医院生存的不良结局。因此,不应仅因ACCI高而拒绝ECPR。然而,医院幸存者中高ACCI与2年死亡率高于低ACCI相关,应密切随访高ACCI患者。