Department of Reproductive Medicine, KK Women's and Children's Hospital, Singapore, Singapore.
Duke-NUS Medical School, Singapore, Singapore.
Hum Reprod. 2018 Nov 1;33(11):2141-2149. doi: 10.1093/humrep/dey300.
Are higher overall and central adiposity associated with reduced fecundability, measured by time-to-pregnancy (TTP), in Asian women?
Higher overall adiposity, but not central adiposity, was associated with longer TTP in Asian women.
High body mass index (BMI) has been associated with a longer TTP, although the associations of body composition and distribution with TTP are less clear. There are no previous studies of TTP in Asian women, who have a relatively higher percentage of body fat and abdominal fat at relatively lower BMI.
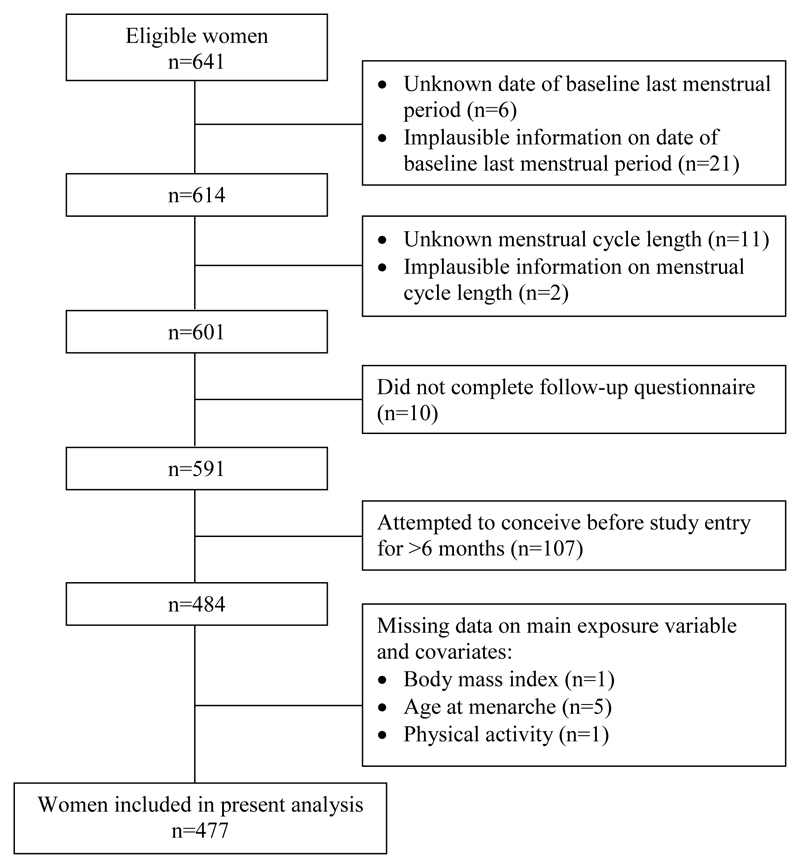
STUDY DESIGN, SIZE, DURATION: Prospective preconception cohort using data from 477 Asian (Chinese, Malay and Indian) women who were planning to conceive and enrolled in the Singapore PREconception Study of long-Term maternal and child Outcomes (S-PRESTO) study, 2015-2017.
PARTICIPANTS/MATERIALS, SETTING, METHODS: Women's mean age was 30.7 years. Overall adiposity was assessed by BMI, sum of 4-site skinfold thicknesses (SFT) and total body fat percentage (TBF%, measured using air displacement plethysmography); central adiposity was assessed by waist circumference (WC), waist-to-hip ratio (WHR), waist-to-height ratio (WHtR) and A body Shape Index (ABSI). Pregnancy occurring within one year from recruitment was ascertained by ultrasonography. Those who did not conceive within one year of recruitment, were lost to follow-up, or initiated fertility treatment were censored. TTP was measured in cycles. Discrete-time proportional hazards models were used to estimate the fecundability ratio (FR) and 95% confidence interval (CI) for each anthropometric measure in association with fecundability, adjusting for confounders.
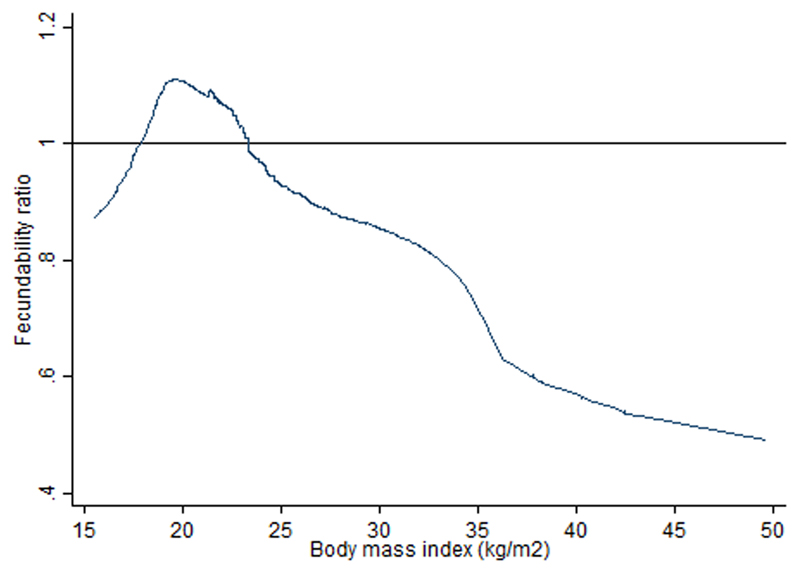
Compared to women with a normal BMI of 18.5-22.9 kg/m2, women with higher BMI of 23-27.4 and ≥27.5 kg/m2 showed lower FR of 0.66 (95% CI 0.45, 0.97) and 0.53 (0.31, 0.89), respectively. Compared to women in the lowest quartile of SFT (25-52.9 mm), those in the highest quartile of ≥90.1 mm showed lower FR of 0.58 (95% CI 0.36, 0.95). Compared to women in the lowest quartile of TBF% (13.6-27.2%), those in the upper two quartiles of 33.0-39.7% and ≥39.8% showed lower FR of 0.56 (95% CI 0.32, 0.98) and 0.43 (0.24, 0.80), respectively. Association of high BMI with reduced fecundability was particularly evident among nulliparous women. Measures of central adiposity (WC, WHR, WHtR, ABSI) were not associated with fecundability.
Small sample size could restrict power of analysis.The analysis was confined to planned pregnancies, which could limit generalizability of findings to non-planned pregnancies, estimated at around 44% in Singapore. Information on the date of last menstrual period for each month was not available, hence the accuracy of self-reported menstrual cycle length could not be validated, potentially introducing error into TTP estimation. Measures of exposures and covariates such as cycle length were not performed repeatedly over time; cycle length might have changed during the period before getting pregnant.
Other than using BMI as the surrogate measure of body fat, we provide additional evidence showing that higher amounts of subcutaneous fat that based on the measure of SFT at the sites of biceps, triceps, suprailiac and subscapular, and TBF% are associated with longer TTP. Achieving optimal weight and reducing total percentage body fat may be a potential intervention target to improve female fertility. The null results observed between central adiposity and TTP requires confirmation in further studies.
STUDY FUNDING/COMPETING INTEREST(S): This research is supported by Singapore National Research Foundation under its Translational and Clinical Research Flagship Programme and administered by the Singapore Ministry of Health's National Medical Research Council, (NMRC/TCR/004-NUS/2008; NMRC/TCR/012-NUHS/2014). Additional funding is provided by the Singapore Institute for Clinical Sciences, Agency for Science Technology and Research (A*STAR), Singapore. Y.S.C., K.M.G., F.Y. and Y.S.L. have received reimbursement to speak at conferences sponsored by companies selling nutritional products. Y.S.C., K.M.G. and S.Y.C. are part of an academic consortium that has received research funding from Abbott, Nutrition, Nestle and Danone. Other authors declared no conflicts of interest.
N/A.
全身和中心性肥胖与亚洲女性的妊娠时间(TTP)呈负相关吗?
全身肥胖与亚洲女性的 TTP 较长有关,而中心性肥胖与 TTP 无关。
高体重指数(BMI)与 TTP 较长有关,尽管身体成分和分布与 TTP 的关系尚不明确。亚洲女性的 BMI 相对较低,但体脂和腹部脂肪的百分比相对较高,因此之前没有关于 TTP 的研究。
研究设计、规模、持续时间:前瞻性孕前队列研究,纳入了 2015 年至 2017 年期间计划怀孕并参加新加坡长期母婴结局研究(S-PRESTO)的 477 名亚洲(华人、马来人和印度人)女性,这些女性的平均年龄为 30.7 岁。全身肥胖通过 BMI、4 点皮褶厚度总和(SFT)和全身脂肪百分比(TBF%,通过空气置换体描记法测量)进行评估;中心性肥胖通过腰围(WC)、腰臀比(WHR)、腰高比(WHtR)和 A 体型指数(ABSI)进行评估。通过超声检查确定一年内是否怀孕。对于一年内未怀孕、失访或开始生育治疗的女性进行了删失。TTP 以周期为单位进行测量。离散时间比例风险模型用于估计每个人体测量指标与生育能力的相关性,调整混杂因素后得出生育能力比值(FR)和 95%置信区间(CI)。
与 BMI 正常(18.5-22.9kg/m2)的女性相比,BMI 较高(23-27.4kg/m2 和≥27.5kg/m2)的女性 FR 分别为 0.66(95%CI 0.45,0.97)和 0.53(0.31,0.89),较低。与 SFT 最低四分位数(25-52.9mm)的女性相比,SFT 最高四分位数(≥90.1mm)的女性 FR 为 0.58(95%CI 0.36,0.95),较低。与 TBF%最低四分位数(13.6-27.2%)的女性相比,TBF%处于上两个四分位数(33.0-39.7%和≥39.8%)的女性 FR 分别为 0.56(95%CI 0.32,0.98)和 0.43(0.24,0.80),较低。BMI 与生育能力下降之间的关联在未生育的女性中尤为明显。中心性肥胖的指标(WC、WHR、WHtR、ABSI)与生育能力无关。
样本量小可能限制了分析的能力。该分析仅限于计划怀孕,这可能限制了发现对非计划怀孕的普遍性,新加坡约有 44%的怀孕属于非计划怀孕。由于每个月的最后一次月经日期信息不可用,因此无法验证自我报告的月经周期长度的准确性,这可能会导致 TTP 估计出现误差。暴露和协变量的测量(如周期长度)没有随时间重复进行;在怀孕前的这段时间里,周期长度可能会发生变化。
除了使用 BMI 作为体脂的替代测量指标外,我们还提供了额外的证据,表明基于肱二头肌、肱三头肌、髂前上棘和肩胛下等部位的 SFT 以及 TBF%测量的皮下脂肪量与 TTP 较长有关。实现理想体重和减少全身脂肪百分比可能是提高女性生育能力的潜在干预目标。中心性肥胖与 TTP 之间的阴性结果需要在进一步的研究中进行证实。
研究资金/利益冲突:本研究得到新加坡国家研究基金会(NRF)转化和临床研究旗舰计划以及新加坡卫生部国家医学研究理事会(NMRC)的支持,(NMRC/TCR/004-NUS/2008;NMRC/TCR/012-NUHS/2014)。额外的资金由新加坡临床科学研究所(ASTAR)和新加坡科学技术研究局(ASTAR)提供。Y.S.C.、K.M.G. 和 F.Y. 因在会议上发表演讲而获得公司销售营养产品的报酬。Y.S.C.、K.M.G. 和 S.Y.C. 是一个学术联盟的成员,该联盟已从雅培、雀巢和达能等公司获得研究资金。其他作者没有利益冲突。
无。