Dr. Yen's Clinic, Taoyuan City, Taiwan.
Management Office for Health Data, China Medical University Hospital, Taichung, Taiwan.
PLoS One. 2018 Oct 4;13(10):e0204859. doi: 10.1371/journal.pone.0204859. eCollection 2018.
Few studies have investigated the therapeutic effects of metformin in patients with type 2 diabetes mellitus (T2DM) and chronic obstructive pulmonary disease (COPD). We compared the risk of all-cause mortality between metformin users and nonusers.
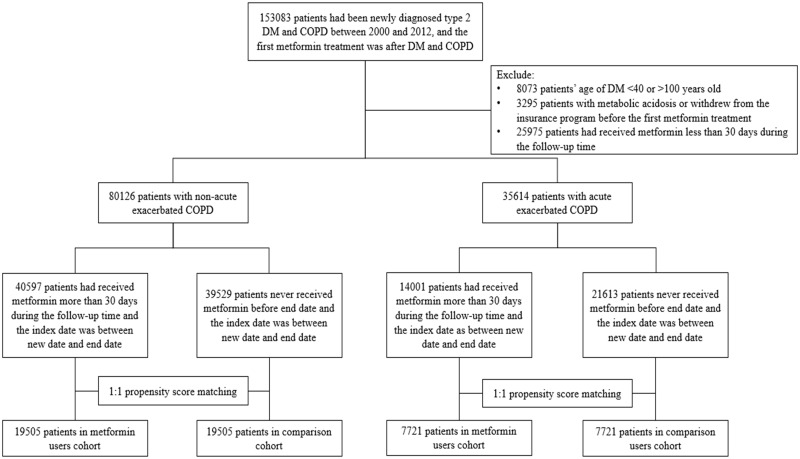
We conducted a retrospective cohort study for patients with T2DM and COPD who were enrolled between January 1, 2000 and June 30, 2012. Individuals with exacerbated symptoms who were hospitalized or sent to the emergency department (ED) were identified as having exacerbated COPD; outpatient claims were identified as having stable COPD. A total of 40,597 metformin users and 39,529 nonusers comprised the cohort of stable COPD; 14,001 metformin users and 21,613 nonusers comprised the cohort of exacerbated COPD. Users and nonusers were matched using propensity score (1:1). Our primary outcome was all-cause mortality.
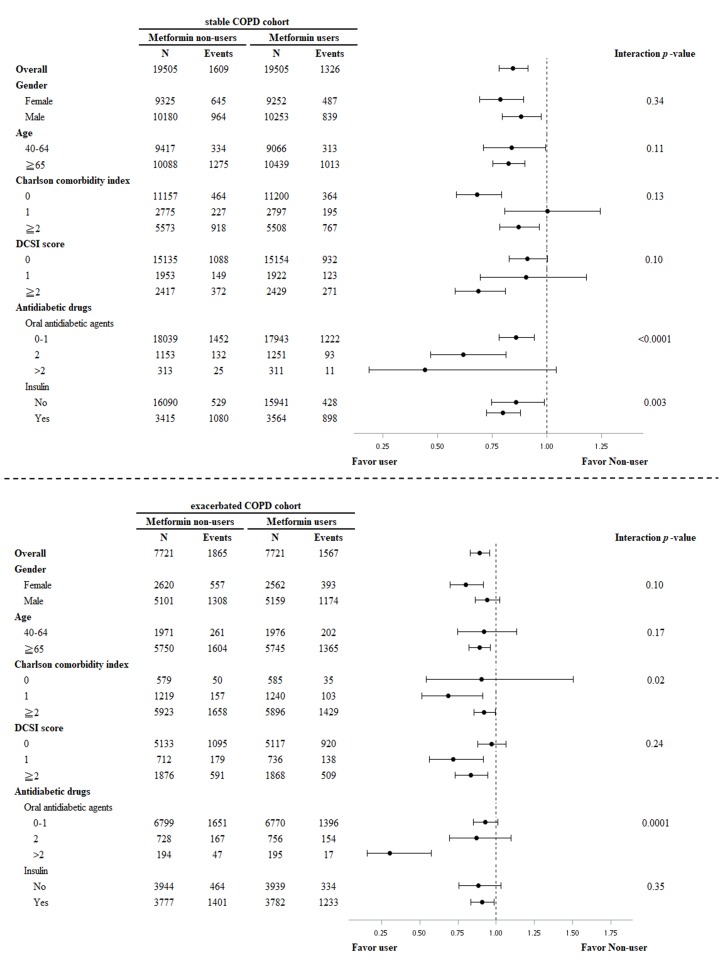
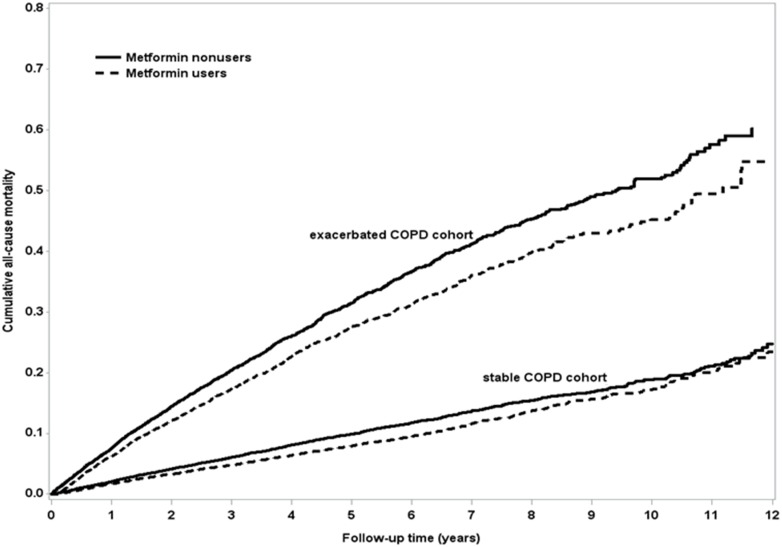
A total of 19,505 metformin users were matched to 19,505 nonusers in the cohort of diabetes with stable COPD. The mean follow-up time was 3.91 years. All-cause mortality was reported in 1326 and 1609 metformin users and nonusers, respectively. After multivariate adjustment, metformin users had lower risk of mortality (adjusted hazard ratio [aHR] = 0.84, p < 0.0001). Metformin users had significantly lower risk of noncardiovascular death (aHR = 0.86, p = 0.0008). A total of 7721 metformin users were matched to 7721 nonusers in the cohort of diabetes with exacerbated COPD. The mean follow-up time was 3.18 years. All-cause mortality was reported in 1567 and 1865 metformin users and nonusers, respectively. After multivariate adjustment, metformin users had significantly lower risk of mortality (aHR = 0.89, p = 0.002) and cardiovascular death (aHR = 0.70, p = 0.01).
This large-series, nationwide cohort study demonstrated that metformin use could significantly lower the risk of all-cause mortality in patients with T2DM and either stable or exacerbated COPD.
很少有研究调查二甲双胍在 2 型糖尿病(T2DM)和慢性阻塞性肺疾病(COPD)患者中的治疗效果。我们比较了使用二甲双胍和未使用二甲双胍的患者的全因死亡率风险。
我们进行了一项回顾性队列研究,纳入了 2000 年 1 月 1 日至 2012 年 6 月 30 日期间患有 T2DM 和 COPD 的患者。住院或被送往急诊部(ED)的症状加重的患者被诊断为 COPD 加重;门诊就诊被诊断为稳定型 COPD。共有 40597 名使用二甲双胍的患者和 39529 名未使用二甲双胍的患者组成稳定型 COPD 队列;14001 名使用二甲双胍的患者和 21613 名未使用二甲双胍的患者组成 COPD 加重队列。使用倾向评分(1:1)对使用者和非使用者进行匹配。我们的主要结局是全因死亡率。
在稳定型 COPD 合并糖尿病队列中,共有 19505 名使用二甲双胍的患者与 19505 名未使用二甲双胍的患者匹配。平均随访时间为 3.91 年。分别有 1326 名和 1609 名使用二甲双胍的患者和非使用者报告了全因死亡。多变量调整后,使用二甲双胍的患者死亡风险较低(调整后的危险比[aHR] = 0.84,p < 0.0001)。使用二甲双胍的患者非心血管死亡风险显著降低(aHR = 0.86,p = 0.0008)。在 COPD 加重合并糖尿病队列中,共有 7721 名使用二甲双胍的患者与 7721 名未使用二甲双胍的患者匹配。平均随访时间为 3.18 年。分别有 1567 名和 1865 名使用二甲双胍的患者和非使用者报告了全因死亡。多变量调整后,使用二甲双胍的患者死亡风险显著降低(aHR = 0.89,p = 0.002)和心血管死亡风险(aHR = 0.70,p = 0.01)。
这项大规模的全国性队列研究表明,在患有 T2DM 且稳定或加重的 COPD 的患者中,使用二甲双胍可显著降低全因死亡率风险。