Head and Neck Unit, Royal Marsden Hospital, London, United Kingdom.
The Institute of Cancer Research Clinical Trials and Statistics Unit, The Institute of Cancer Research, London, United Kingdom.
Eur J Cancer. 2018 Nov;103:249-258. doi: 10.1016/j.ejca.2018.08.006. Epub 2018 Oct 1.
About 40-60% of patients treated with post-operative radiotherapy for parotid cancer experience ipsilateral sensorineural hearing loss. Intensity-modulated radiotherapy (IMRT) can reduce radiation dose to the cochlea. COSTAR, a phase III trial, investigated the role of cochlear-sparing IMRT (CS-IMRT) in reducing hearing loss.
Patients (pT1-4 N0-3 M0) were randomly assigned (1:1) to 3-dimensional conformal radiotherapy (3DCRT) or CS-IMRT by minimisation, balancing for centre and radiation dose of 60Gy or 65Gy in 30 daily fractions. The primary end-point was proportion of patients with sensorineural hearing loss in the ipsilateral cochlea of ≥10 dB bone conduction at 4000 Hz 12 months after radiotherapy compared using Fisher's exact test. Secondary end-points included hearing loss at 6 and 24 months, balance assessment, acute and late toxicity, patient-reported quality of life, time to recurrence and survival.
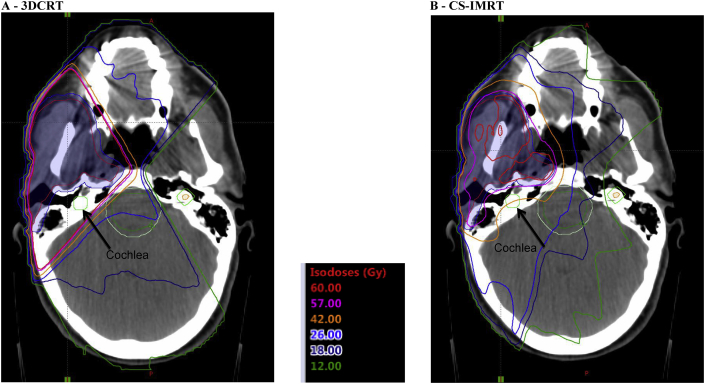
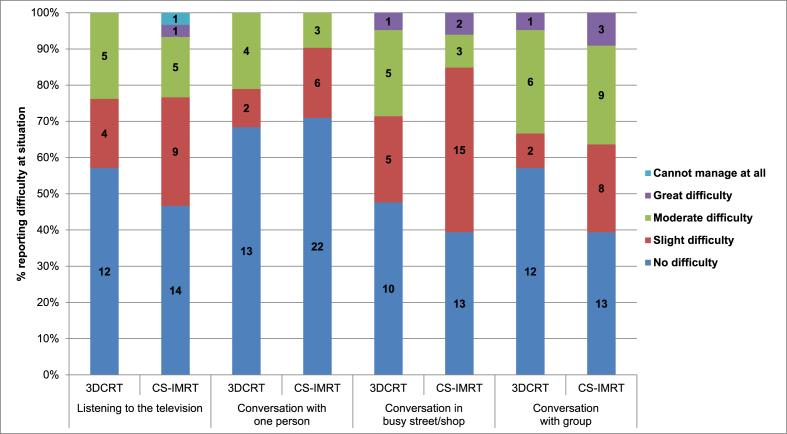
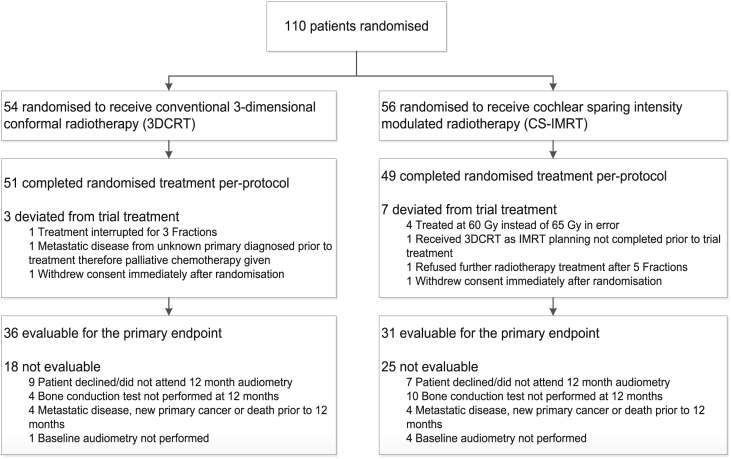
From Aug 2008 to Feb 2013, 110 patients (54 3DCRT; 56 CS-IMRT) were enrolled from 22 UK centres. Median doses to the ipsilateral cochlea were 3DCRT: 56.2Gy and CS-IMRT: 35.7Gy (p < 0.0001). 67/110 (61%) patients were evaluable for the primary end-point; main reasons for non-evaluability were non-attendance at follow-up or incomplete audiology assessment. At 12 months, 14/36 (39%) 3DCRT and 11/31 (36%) CS-IMRT patients had ≥10 dB loss (p = 0.81). No statistically significant differences were observed in hearing loss at 6 or 24 months or in other secondary end-points including patient-reported hearing outcomes.
CS-IMRT reduced the radiation dose below the accepted tolerance of the cochlea, but this did not lead to a reduction in the proportion of patients with clinically relevant hearing loss.
约 40-60%接受腮腺癌术后放疗的患者会出现同侧感觉神经性听力损失。调强放疗(IMRT)可以降低耳蜗的辐射剂量。COSTAR 是一项 III 期试验,旨在研究保护耳蜗的调强放疗(CS-IMRT)在降低听力损失方面的作用。
患者(pT1-4 N0-3 M0)按 1:1 比例通过最小化法随机分配至 3 维适形放疗(3DCRT)或 CS-IMRT 组,按中心和 60Gy 或 65Gy(30 次分割)的剂量平衡分组。主要终点为放疗后 12 个月时同侧耳蜗骨导 4000Hz 听力损失≥10dB 的患者比例,采用 Fisher 确切检验进行比较。次要终点包括 6 个月和 24 个月时的听力损失、平衡评估、急性和迟发性毒性、患者报告的生活质量、复发和生存时间。
2008 年 8 月至 2013 年 2 月,来自英国 22 个中心的 110 例患者(54 例 3DCRT;56 例 CS-IMRT)入组。同侧耳蜗的中位剂量为 3DCRT:56.2Gy,CS-IMRT:35.7Gy(p<0.0001)。110 例患者中有 67 例(61%)可评估主要终点;主要失访原因是未参加随访或未完成听力学评估。12 个月时,3DCRT 组 36 例中有 14 例(39%)、CS-IMRT 组 31 例中有 11 例(36%)出现≥10dB 的听力损失(p=0.81)。6 个月和 24 个月时的听力损失或其他次要终点(包括患者报告的听力结局)无统计学显著差异。
CS-IMRT 将辐射剂量降低至耳蜗可接受的耐受水平以下,但这并未导致出现具有临床意义的听力损失的患者比例降低。