Head and Neck Unit, Royal Marsden Hospitals NHS Foundation Trust, London, UK.
Lancet Oncol. 2011 Feb;12(2):127-36. doi: 10.1016/S1470-2045(10)70290-4. Epub 2011 Jan 12.
Xerostomia is the most common late side-effect of radiotherapy to the head and neck. Compared with conventional radiotherapy, intensity-modulated radiotherapy (IMRT) can reduce irradiation of the parotid glands. We assessed the hypothesis that parotid-sparing IMRT reduces the incidence of severe xerostomia.
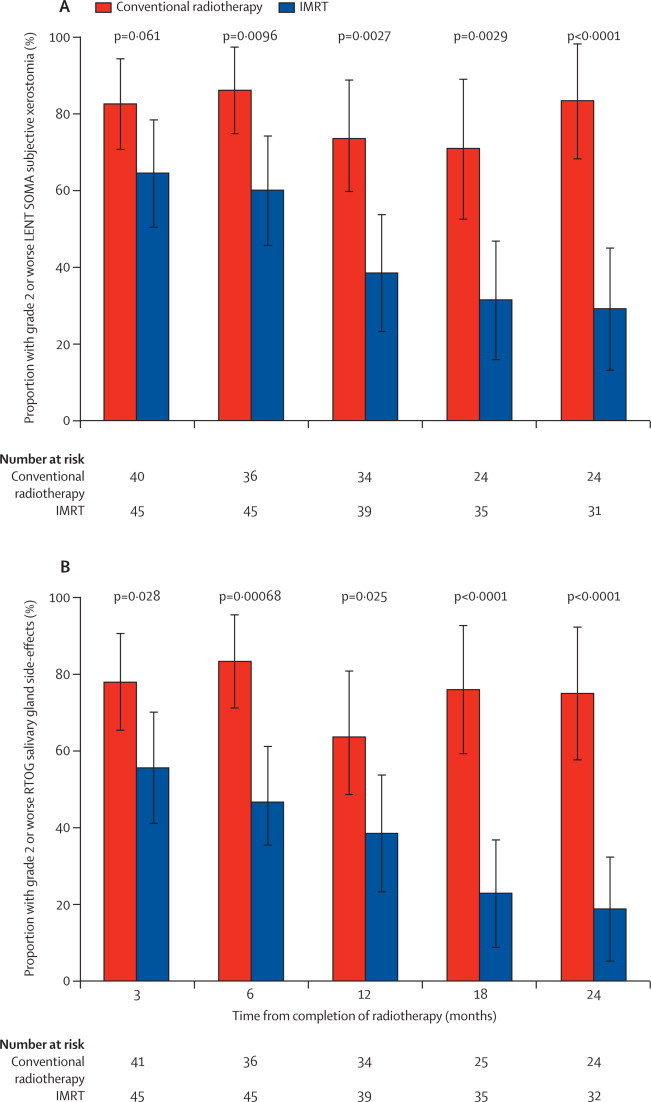
We undertook a randomised controlled trial between Jan 21, 2003, and Dec 7, 2007, that compared conventional radiotherapy (control) with parotid-sparing IMRT. We randomly assigned patients with histologically confirmed pharyngeal squamous-cell carcinoma (T1-4, N0-3, M0) at six UK radiotherapy centres between the two radiotherapy techniques (1:1 ratio). A dose of 60 or 65 Gy was prescribed in 30 daily fractions given Monday to Friday. Treatment was not masked. Randomisation was by computer-generated permuted blocks and was stratified by centre and tumour site. Our primary endpoint was the proportion of patients with grade 2 or worse xerostomia at 12 months, as assessed by the Late Effects of Normal Tissue (LENT SOMA) scale. Analyses were done on an intention-to-treat basis, with all patients who had assessments included. Long-term follow-up of patients is ongoing. This study is registered with the International Standard Randomised Controlled Trial register, number ISRCTN48243537.
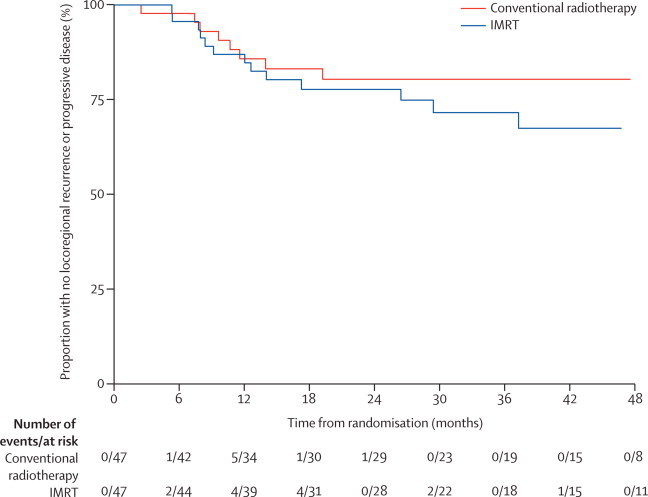
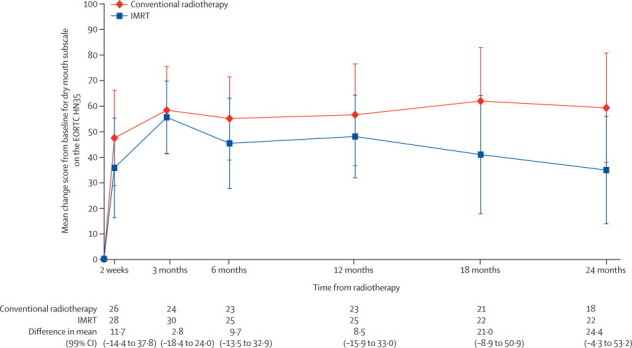
47 patients were assigned to each treatment arm. Median follow-up was 44·0 months (IQR 30·0-59·7). Six patients from each group died before 12 months and seven patients from the conventional radiotherapy and two from the IMRT group were not assessed at 12 months. At 12 months xerostomia side-effects were reported in 73 of 82 alive patients; grade 2 or worse xerostomia at 12 months was significantly lower in the IMRT group than in the conventional radiotherapy group (25 [74%; 95% CI 56-87] of 34 patients given conventional radiotherapy vs 15 [38%; 23-55] of 39 given IMRT, p=0·0027). The only recorded acute adverse event of grade 2 or worse that differed significantly between the treatment groups was fatigue, which was more prevalent in the IMRT group (18 [41%; 99% CI 23-61] of 44 patients given conventional radiotherapy vs 35 [74%; 55-89] of 47 given IMRT, p=0·0015). At 24 months, grade 2 or worse xerostomia was significantly less common with IMRT than with conventional radiotherapy (20 [83%; 95% CI 63-95] of 24 patients given conventional radiotherapy vs nine [29%; 14-48] of 31 given IMRT; p<0·0001). At 12 and 24 months, significant benefits were seen in recovery of saliva secretion with IMRT compared with conventional radiotherapy, as were clinically significant improvements in dry-mouth-specific and global quality of life scores. At 24 months, no significant differences were seen between randomised groups in non-xerostomia late toxicities, locoregional control, or overall survival.
Sparing the parotid glands with IMRT significantly reduces the incidence of xerostomia and leads to recovery of saliva secretion and improvements in associated quality of life, and thus strongly supports a role for IMRT in squamous-cell carcinoma of the head and neck.
Cancer Research UK (CRUK/03/005).

口干症是头颈部放疗最常见的晚期副作用。与常规放疗相比,调强放疗(IMRT)可以减少腮腺的照射。我们假设保腮腺的调强放疗可以降低严重口干症的发生率。
我们在 2003 年 1 月 21 日至 2007 年 12 月 7 日期间进行了一项随机对照试验,比较了常规放疗(对照组)与保腮腺的调强放疗。我们在六个英国放疗中心将经组织学证实的咽鳞癌(T1-4、N0-3、M0)患者随机分配到两种放疗技术中(1:1 比例)。在周一至周五给予 30 天 60 或 65Gy 的剂量。治疗未进行屏蔽。随机分组采用计算机生成的随机分组和按中心和肿瘤部位分层。我们的主要终点是在 12 个月时,根据晚期正常组织效应(LENT SOMA)量表评估的 2 级或更严重口干症的患者比例。分析采用意向治疗原则,所有接受评估的患者均包括在内。正在对患者进行长期随访。该研究在国际标准随机对照试验注册中心注册,注册号为 ISRCTN48243537。
每组 47 例患者接受了治疗。中位随访时间为 44.0 个月(IQR 30.0-59.7)。每组各有 6 例患者在 12 个月前死亡,7 例常规放疗组和 2 例调强放疗组的患者在 12 个月时未进行评估。在 12 个月时,82 例存活患者中有 73 例报告了口干副作用;12 个月时,调强放疗组的口干症 2 级或更严重的比例明显低于常规放疗组(常规放疗组 34 例患者中有 25 例[74%;95%CI 56-87],调强放疗组 39 例患者中有 15 例[38%;23-55],p=0.0027)。两组之间唯一记录的 2 级或更严重的急性不良事件是疲劳,调强放疗组更为常见(常规放疗组 44 例患者中有 18 例[41%;99%CI 23-61],调强放疗组 47 例患者中有 35 例[74%;55-89],p=0.0015)。24 个月时,调强放疗组的口干症 2 级或更严重的比例明显低于常规放疗组(常规放疗组 24 例患者中有 20 例[83%;95%CI 63-95],调强放疗组 31 例患者中有 9 例[29%;14-48],p<0.0001)。在 12 个月和 24 个月时,与常规放疗相比,调强放疗在恢复唾液分泌方面具有显著优势,并且在口干特异性和总体生活质量评分方面也有显著改善。24 个月时,两组之间在非口干症晚期毒性、局部区域控制或总体生存率方面无显著差异。
调强放疗保腮腺可显著降低口干症的发生率,并促进唾液分泌的恢复和相关生活质量的改善,因此强烈支持调强放疗在头颈部鳞状细胞癌中的作用。
英国癌症研究中心(CRUK/03/005)。