Lazarus Jeffrey V, Mozalevskis Antons, Safreed-Harmon Kelly, Eramova Irina
1CHIP, Centre for Health and Infectious Disease Research and WHO Collaborating Centre on HIV and Viral Hepatitis, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark.
2World Health Organization (WHO) Regional Office for Europe, Copenhagen, Denmark.
Hepatol Med Policy. 2016 Jun 30;1:3. doi: 10.1186/s41124-016-0009-5. eCollection 2016.
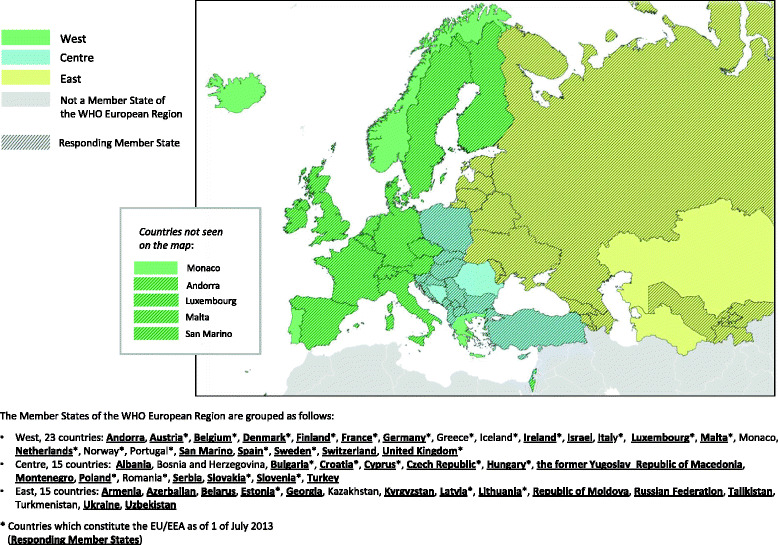
Hepatitis B and C are major public health threats in the World Health Organization (WHO) European Region. Viral hepatitis surveillance shortcomings have resulted in many WHO Member States having insufficient data available to guide decision-making. This study describes surveillance in the region based on a quantitative sub-analysis of findings from the 2013 WHO viral hepatitis policy report and a qualitative analysis of civil society survey responses associated with these findings.
Descriptive statistics were created from information that national government focal points for viral hepatitis in 44 countries had previously reported in response to the WHO survey. Bivariate analysis was performed to compare data from within and outside of the European Union/European Economic Area (EU/EEA). Survey responses from civil society organizations in the countries of the WHO European Region were collated, and a descriptive analysis of the comments on surveillance-related questions was performed to identify key themes.
The response rate for the survey of governments was 83 % among both EU/EEA countries (25/30) and non-EU/EEA countries (19/23). More than 90 % of governments reported having national surveillance systems for the acute forms of hepatitis B and hepatitis C, but less than two-thirds reported surveillance for the chronic forms of both diseases. High proportions of governments reported having central registries for the reporting of deaths (96 %) and liver cancer cases (80 %), while less than half reported regularly conducting viral hepatitis sero-surveys. All responding Member States reported having adequate laboratory capacity nationally to support hepatitis outbreak investigations and other surveillance activities. Target populations for sero-surveys most commonly included people who inject drugs (27 %), the general population (25 %), men who have sex with men (20 %) and pregnant women (20 %). Few statistically significant differences were found between EU/EEA and non-EU/EEA countries.
Study findings indicated a capacity for robust viral hepatitis surveillance across the WHO European Region, with most countries having important surveillance components in place, but notable weaknesses were also identified. There is an urgent need for countries throughout the region to strengthen their surveillance programs in order to maximize the population-level impact of advances in HBV and HCV prevention and treatment.
乙型和丙型肝炎是世界卫生组织(WHO)欧洲区域面临的重大公共卫生威胁。病毒性肝炎监测存在缺陷,导致许多WHO成员国缺乏足够数据来指导决策。本研究基于对2013年WHO病毒性肝炎政策报告结果的定量子分析以及与这些结果相关的民间社会调查答复的定性分析,描述了该区域的监测情况。
描述性统计数据来自44个国家的国家政府病毒性肝炎联络点先前针对WHO调查所报告的信息。进行双变量分析以比较欧盟/欧洲经济区(EU/EEA)内外的数据。整理了WHO欧洲区域各国民间社会组织的调查答复,并对与监测相关问题的评论进行了描述性分析,以确定关键主题。
在EU/EEA国家(25/30)和非EU/EEA国家(19/23)中,政府调查的答复率均为83%。超过90%的政府报告称拥有针对急性乙型和丙型肝炎的国家监测系统,但报告针对这两种疾病慢性形式进行监测的政府不到三分之二。高比例的政府报告称设有用于报告死亡(96%)和肝癌病例(80%)的中央登记处,而报告定期开展病毒性肝炎血清学调查的政府不到一半。所有作出答复的成员国均报告称本国具备足够的实验室能力以支持肝炎疫情调查和其他监测活动。血清学调查的目标人群最常见的包括注射吸毒者(27%)、普通人群(25%)、男男性行为者(20%)和孕妇(20%)。在EU/EEA国家和非EU/EEA国家之间未发现统计学上的显著差异。
研究结果表明WHO欧洲区域具备开展强有力的病毒性肝炎监测的能力,大多数国家已具备重要的监测组成部分,但也发现了明显的薄弱环节。该区域各国迫切需要加强其监测计划,以最大限度地提高乙肝和丙肝预防与治疗进展对人群层面的影响。