Department of Infectious Diseases, Hospital Universitari de Bellvitge, Institut d'Investigació Biomèdica de Bellvitge (IDIBELL), Feixa Llarga s/n, 08907 L'Hospitalet de Llobregat, Barcelona, Spain.
VINCat Program, Barcelona, Spain.
BMC Infect Dis. 2018 Oct 5;18(1):507. doi: 10.1186/s12879-018-3413-1.
Healthcare-associated infections caused by Pseudomonas aeruginosa are associated with poor outcomes. However, the role of P. aeruginosa in surgical site infections after colorectal surgery has not been evaluated. The aim of this study was to determine the predictive factors and outcomes of surgical site infections caused by P. aeruginosa after colorectal surgery, with special emphasis on the role of preoperative oral antibiotic prophylaxis.
We conducted an observational, multicenter, prospective cohort study of all patients undergoing elective colorectal surgery at 10 Spanish hospitals (2011-2014). A logistic regression model was used to identify predictive factors for P. aeruginosa surgical site infections.
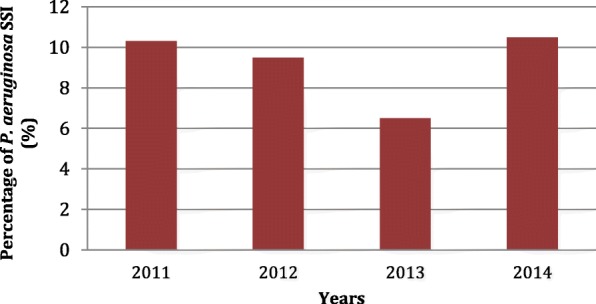
Out of 3701 patients, 669 (18.1%) developed surgical site infections, and 62 (9.3%) of these were due to P. aeruginosa. The following factors were found to differentiate between P. aeruginosa surgical site infections and those caused by other microorganisms: American Society of Anesthesiologists' score III-IV (67.7% vs 45.5%, p = 0.001, odds ratio (OR) 2.5, 95% confidence interval (95% CI) 1.44-4.39), National Nosocomial Infections Surveillance risk index 1-2 (74.2% vs 44.2%, p < 0.001, OR 3.6, 95% CI 2.01-6.56), duration of surgery ≥75thpercentile (61.3% vs 41.4%, p = 0.003, OR 2.2, 95% CI 1.31-3.83) and oral antibiotic prophylaxis (17.7% vs 33.6%, p = 0.01, OR 0.4, 95% CI 0.21-0.83). Patients with P. aeruginosa surgical site infections were administered antibiotic treatment for a longer duration (median 17 days [interquartile range (IQR) 10-24] vs 13d [IQR 8-20], p = 0.015, OR 1.1, 95% CI 1.00-1.12), had a higher treatment failure rate (30.6% vs 20.8%, p = 0.07, OR 1.7, 95% CI 0.96-2.99), and longer hospitalization (median 22 days [IQR 15-42] vs 19d [IQR 12-28], p = 0.02, OR 1.1, 95% CI 1.00-1.17) than those with surgical site infections due to other microorganisms. Independent predictive factors associated with P. aeruginosa surgical site infections were the National Nosocomial Infections Surveillance risk index 1-2 (OR 2.3, 95% CI 1.03-5.40) and the use of oral antibiotic prophylaxis (OR 0.4, 95% CI 0.23-0.90).
We observed that surgical site infections due to P. aeruginosa are associated with a higher National Nosocomial Infections Surveillance risk index, poor outcomes, and lack of preoperative oral antibiotic prophylaxis. These findings can aid in establishing specific preventive measures and appropriate empirical antibiotic treatment.
铜绿假单胞菌引起的医源性感染与不良预后相关。然而,在结直肠手术后,铜绿假单胞菌引起的手术部位感染的作用尚未得到评估。本研究旨在确定结直肠手术后由铜绿假单胞菌引起的手术部位感染的预测因素和结果,特别强调术前口服抗生素预防的作用。
我们对 10 家西班牙医院(2011-2014 年)所有接受择期结直肠手术的患者进行了一项观察性、多中心、前瞻性队列研究。使用逻辑回归模型确定铜绿假单胞菌手术部位感染的预测因素。
在 3701 例患者中,669 例(18.1%)发生手术部位感染,其中 62 例(9.3%)为铜绿假单胞菌引起。以下因素可区分铜绿假单胞菌手术部位感染和其他微生物引起的手术部位感染:美国麻醉师协会评分 III-IV(67.7%比 45.5%,p=0.001,优势比(OR)2.5,95%置信区间(95%CI)1.44-4.39)、国家医院感染监测风险指数 1-2(74.2%比 44.2%,p<0.001,OR 3.6,95%CI 2.01-6.56)、手术时间≥75 百分位(61.3%比 41.4%,p=0.003,OR 2.2,95%CI 1.31-3.83)和口服抗生素预防(17.7%比 33.6%,p=0.01,OR 0.4,95%CI 0.21-0.83)。铜绿假单胞菌手术部位感染患者的抗生素治疗时间更长(中位数 17 天[四分位距(IQR)10-24]比 13 天[IQR 8-20],p=0.015,OR 1.1,95%CI 1.00-1.12)、治疗失败率更高(30.6%比 20.8%,p=0.07,OR 1.7,95%CI 0.96-2.99)、住院时间更长(中位数 22 天[IQR 15-42]比 19 天[IQR 12-28],p=0.02,OR 1.1,95%CI 1.00-1.17),而不是其他微生物引起的手术部位感染。与铜绿假单胞菌手术部位感染相关的独立预测因素包括国家医院感染监测风险指数 1-2(OR 2.3,95%CI 1.03-5.40)和口服抗生素预防(OR 0.4,95%CI 0.23-0.90)。
我们观察到,由铜绿假单胞菌引起的手术部位感染与较高的国家医院感染监测风险指数、不良预后和缺乏术前口服抗生素预防有关。这些发现有助于制定特定的预防措施和适当的经验性抗生素治疗。