Medical Intensive Care Unit, Nantes University Hospital, Nantes, France.
Centre for Research in Transplantation and Immunology (CRTI) UMR1064, INSERM, Nantes University, Nantes, France.
Crit Care. 2018 Oct 5;22(1):251. doi: 10.1186/s13054-018-2179-6.
This study investigated changes in plasma level of soluble endothelial protein C receptor (sEPCR) in association with outcome in patients with septic shock. We explored sEPCR for early sepsis prognosis assessment and constructed a scoring system based on clinical and biological data, in order to discriminate between surviving at hospital discharge and non-surviving patients.
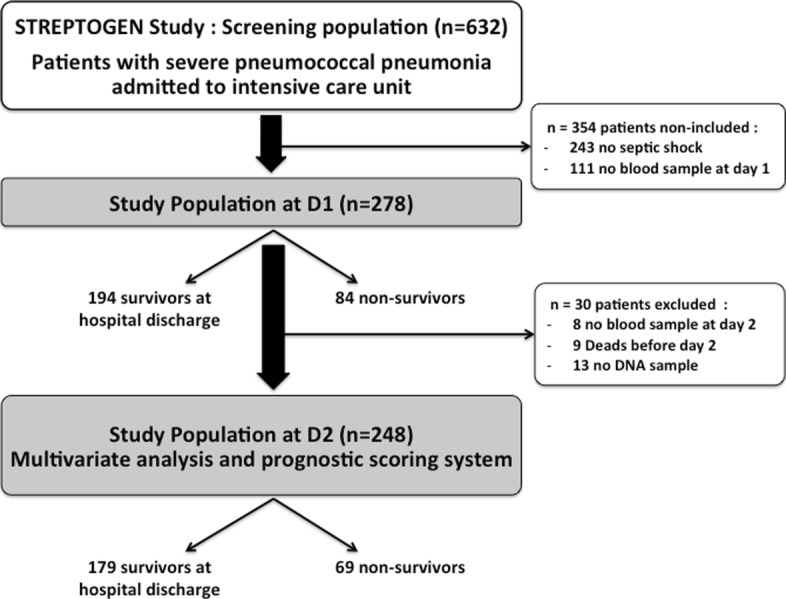
Clinical data and samples were extracted from the prospective "STREPTOGENE" cohort. We enrolled 278 patients, from 50 intensive care units (ICUs), with septic shock caused by pneumococcal pneumonia. Patients were divided into survivors (n = 194) and non-survivors (n = 84) based on in-hospital mortality. Soluble EPCR plasma levels were quantified at day 1 (D1) and day 2 (D2) by ELISA. The EPCR gene A3 haplotype was determined. Patients were followed up until hospital discharge. Univariate and multivariate analyses were performed. A scoring system was constructed using least absolute shrinkage and selection operator (lasso) logistic regression for selecting predictive variables.
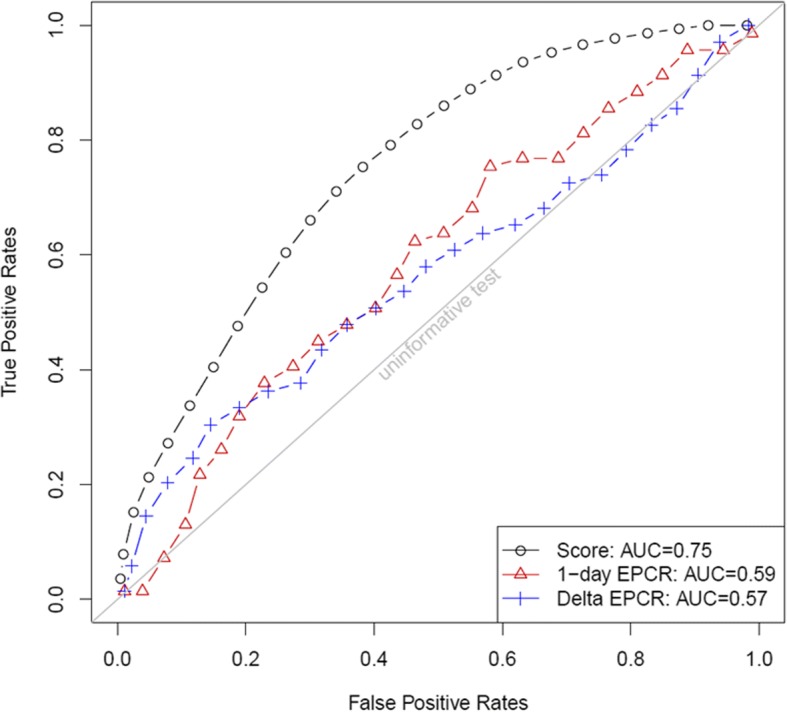
In-hospital mortality was 30.2% (n = 84). Plasma sEPCR level was significantly higher at D1 and D2 in non-surviving patients compared to patients surviving to hospital discharge (p = 0.0447 and 0.0047, respectively). Early increase in sEPCR at D2 was found in non-survivors while a decrease was observed in the survival group (p = 0.0268). EPCR A3 polymorphism was not associated with mortality. Baseline sEPCR level and its variation from D1 to D2 were independent predictors of in-hospital mortality. The scoring system including sEPCR predicted mortality with an AUC of 0.75.
Our findings confirm that high plasma sEPCR and its increase at D2 are associated with poor outcome in sepsis and thus we propose sEPCR as a key player in the pathogenesis of sepsis and as a potential biomarker of sepsis outcome.
本研究旨在探讨脓毒性休克患者血浆可溶性内皮蛋白 C 受体(sEPCR)水平的变化与预后的关系。我们探讨了 sEPCR 用于早期脓毒症预后评估,并构建了一个基于临床和生物学数据的评分系统,以区分出院时存活和非存活患者。
从前瞻性“STREPTOGENE”队列中提取临床数据和样本。我们纳入了 278 名来自 50 个重症监护病房(ICU)的由肺炎链球菌性肺炎引起的脓毒性休克患者。根据院内死亡率将患者分为存活组(n=194)和非存活组(n=84)。通过酶联免疫吸附试验(ELISA)在第 1 天(D1)和第 2 天(D2)定量测定血浆 sEPCR 水平。确定 EPCR 基因 A3 单倍型。对患者进行随访直至出院。进行单变量和多变量分析。使用最小绝对收缩和选择算子(lasso)逻辑回归构建评分系统,用于选择预测变量。
院内死亡率为 30.2%(n=84)。与存活至出院的患者相比,非存活患者的 D1 和 D2 时血浆 sEPCR 水平明显更高(p=0.0447 和 0.0047)。在非存活者中观察到 D2 时 sEPCR 的早期升高,而在存活组中观察到下降(p=0.0268)。EPCR A3 多态性与死亡率无关。基线 sEPCR 水平及其从 D1 到 D2 的变化是院内死亡率的独立预测因子。包括 sEPCR 在内的评分系统预测死亡率的 AUC 为 0.75。
我们的发现证实,高血浆 sEPCR 及其在 D2 时的升高与脓毒症不良预后相关,因此我们提出 sEPCR 是脓毒症发病机制中的关键因素,也是脓毒症预后的潜在生物标志物。