Novo Nordisk Foundation Center for Basic Metabolic Research, Section of Metabolic Genetics, Faculty of Health and Medical Sciences, University of Copenhagen, Blegdamsvej 3B, DK-2200, Copenhagen, Denmark.
Institute for Regional Health Research, University of Southern Denmark, Odense, Denmark.
Diabetologia. 2019 Jan;62(1):147-155. doi: 10.1007/s00125-018-4739-3. Epub 2018 Oct 6.
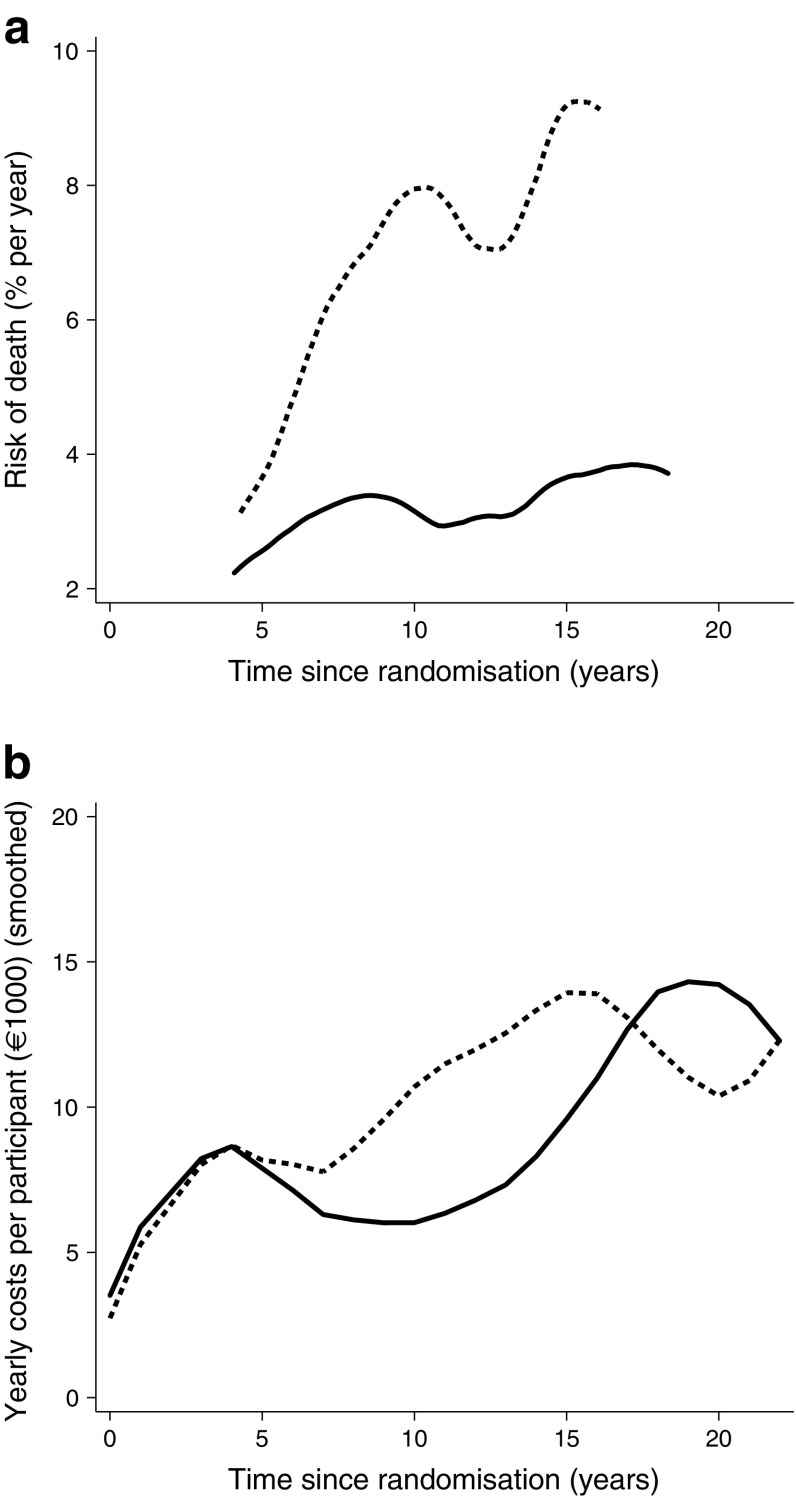
AIMS/HYPOTHESIS: Long-term follow-up of the Steno-2 study demonstrated that intensified multifactorial intervention increased median lifespan by 7.9 years and delayed incident cardiovascular disease by a median of 8.1 years compared with conventional multifactorial intervention during 21.2 years of follow-up. In this post hoc analysis of data from the Steno-2 study, we aimed to study the difference in direct medical costs associated with conventional vs intensified treatment.
In 1993, 160 Danish individuals with type 2 diabetes and microalbuminuria were randomised to conventional or intensified multifactorial target-driven intervention for 7.8 years. Information on direct healthcare costs was retrieved from health registries, and the costs in the two groups of participants were compared by bootstrap t test analysis.
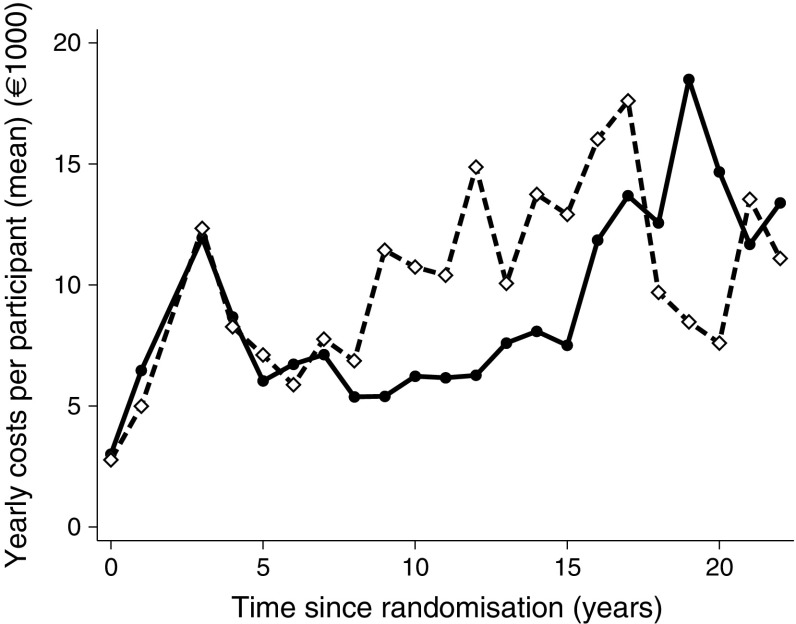
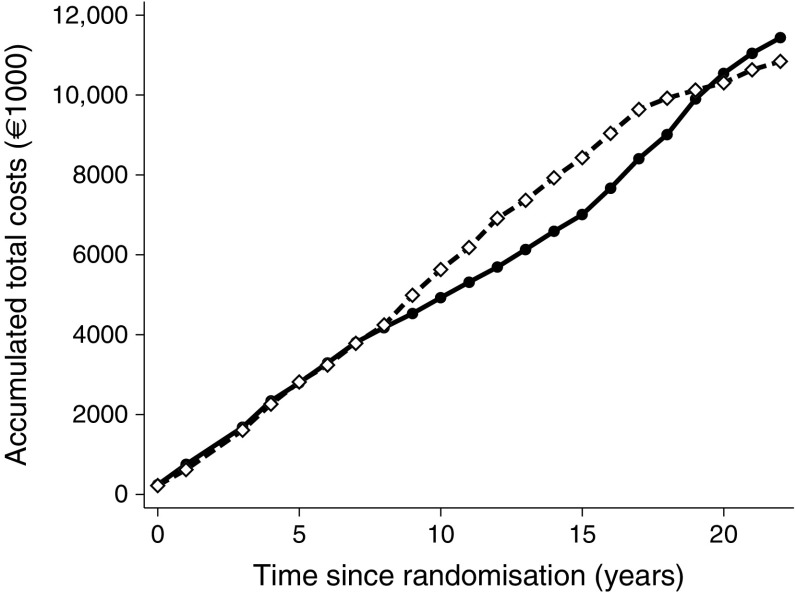
Over 21.2 years of follow-up, there was no difference in total direct medical costs between the intensified treatment group, €12,126,900, and the conventional treatment group, €11,181,700 (p = 0.48). The mean cost per person-year during 1996-2014 was significantly lower in the intensified treatment group (€8725 in the intensive group and €10,091 in the conventional group, p = 0.045). The main driver of this difference was reduced costs associated with inpatient admissions related to cardiovascular disease (p = 0.0024).
CONCLUSIONS/INTERPRETATION: Over a follow-up period of 21.2 years, we found no difference in total costs and reduced cost per person-year associated with intensified multifactorial treatment for 7.8 years compared with conventional multifactorial treatment. Considering the substantial gain in life-years and health benefits achieved with intensified treatment, we conclude that intensified multifaceted intervention in high-risk individuals with type 2 diabetes seems to be highly feasible when balancing healthcare costs and treatment benefits in a Danish healthcare setting.
目的/假设:Steno-2 研究的长期随访结果表明,与常规多因素干预相比,强化多因素干预在 21.2 年的随访期间增加了 7.9 年的中位寿命,并将心血管疾病的发病中位数推迟了 8.1 年。在 Steno-2 研究的数据的这项事后分析中,我们旨在研究常规治疗与强化治疗相关的直接医疗成本差异。
1993 年,160 名患有 2 型糖尿病和微量白蛋白尿的丹麦人被随机分配到常规或强化多因素目标驱动干预组,进行 7.8 年的治疗。直接医疗成本信息从健康登记处检索,通过 bootstrap t 检验分析比较两组参与者的成本。
在 21.2 年的随访期间,强化治疗组的总直接医疗费用为 1212.69 万欧元,常规治疗组为 1118.17 万欧元(p=0.48),两组之间没有差异。1996-2014 年期间,强化治疗组的人均年费用明显较低(强化组为 8725 欧元,常规组为 10091 欧元,p=0.045)。造成这种差异的主要原因是与心血管疾病相关的住院费用降低(p=0.0024)。
结论/解释:在 21.2 年的随访期间,我们发现与常规多因素治疗相比,强化多因素治疗 7.8 年与总费用和人均年费用降低无关。考虑到强化治疗在获得生命年和健康益处方面的显著获益,我们得出结论,在丹麦医疗保健环境中,在平衡医疗成本和治疗效益的情况下,对 2 型糖尿病高危人群进行强化多方面干预似乎是非常可行的。