Health Economics Resource Center and Center for Implementation to Innovation, Veterans Affairs Palo Alto Health Care System, Menlo Park, CA; Perinatal Epidemiology and Health Outcomes Research Unit, Department of Pediatrics, Division of Neonatology, Stanford University School of Medicine, Stanford, CA.
Health Economics Resource Center and Center for Implementation to Innovation, Veterans Affairs Palo Alto Health Care System, Menlo Park, CA; Perinatal Epidemiology and Health Outcomes Research Unit, Department of Pediatrics, Division of Neonatology, Stanford University School of Medicine, Stanford, CA.
J Pediatr. 2019 Jan;204:118-125.e14. doi: 10.1016/j.jpeds.2018.08.041. Epub 2018 Oct 5.
To provide population-based estimates of the hospital-related costs of maternal and newborn care, and how these vary by gestational age and birth weight.
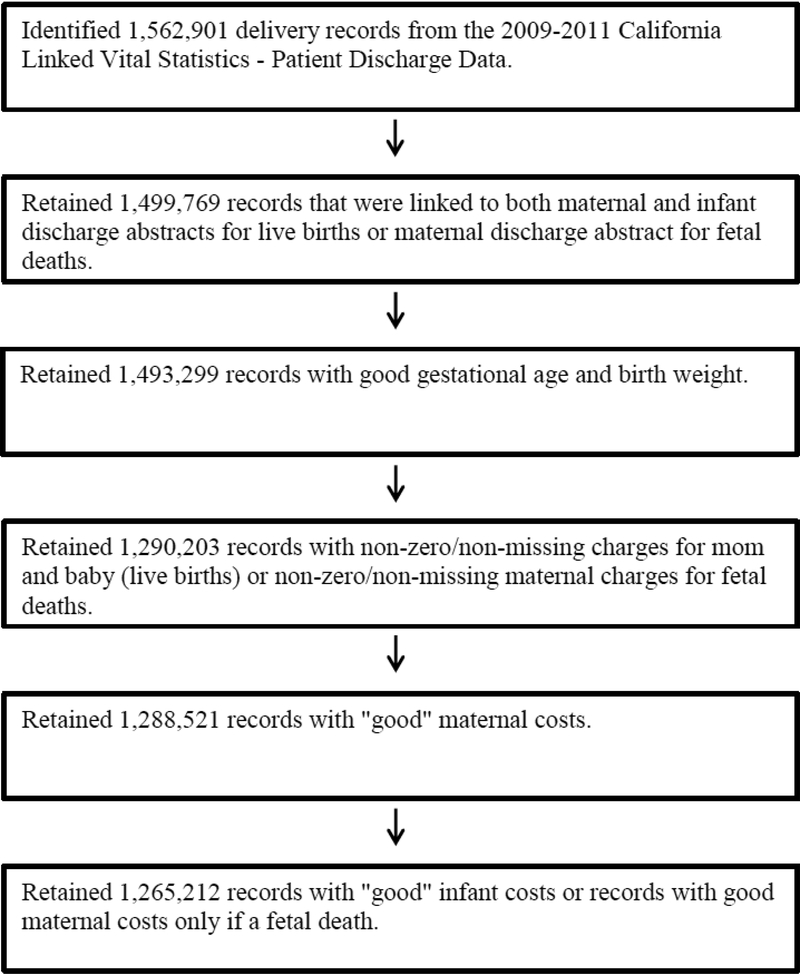
We conducted a retrospective analysis of 2009-2011 California in-hospital deliveries at nonfederal hospitals with the infant and maternal discharge data successfully (96%) linked to birth certificates. Cost-to-charge ratios were used to estimate costs from charges. Physician hospital payments were estimated by mean diagnosis related group-specific reimbursement and costs were adjusted for inflation to December 2017 values. After exclusions for incomplete or missing data, the final sample was 1 265 212.
The mean maternal costs for all in-hospital deliveries was $8204, increasing to $13 154 for late preterm (32-36 weeks) and $22 702 for very preterm (<32 weeks) mothers. The mean cost for all newborns was $6389: $2433 for term infants, $22 102 for late preterm, $223 931 for very preterm infants, and $317 982 for extremely preterm infants (<28 weeks). Preterm infants were 8.1% of cases but incurred 60.9% of costs; for very preterm and extremely preterm infants, these shares were 1.0% and 36.5%, and 0.4% and 20.0%, respectively. Overall, mothers incurred 56% of the total costs during the delivery hospitalization.
Both maternal and neonatal costs are skewed, with this being much more pronounced for infants. Preterm birth is much more expensive than term delivery, with the additional costs predominately incurred by the infants. The small share of infants who require extensive stays in neonatal intensive care incur a large share of neonatal costs and these costs have increased over time.
提供基于人群的孕产妇和新生儿护理相关住院费用估计,并展示这些费用如何随胎龄和出生体重而变化。
我们对 2009 年至 2011 年在非联邦医院分娩的加利福尼亚住院分娩进行了回顾性分析,这些医院的婴儿和产妇出院数据与出生证明成功(96%)相关联。使用成本与收费比率来根据收费估计成本。通过平均诊断相关组特定报销来估算医师医院支付费用,并将成本调整为 2017 年 12 月的通胀率。在排除不完整或缺失数据后,最终样本量为 1 265 212 例。
所有住院分娩的产妇平均费用为 8204 美元,晚期早产儿(32-36 周)为 13154 美元,极早产儿(<32 周)为 22702 美元。所有新生儿的平均费用为 6389 美元:足月婴儿为 2433 美元,晚期早产儿为 22102 美元,极早产儿为 223931 美元,超早产儿(<28 周)为 317982 美元。早产儿占病例的 8.1%,但占费用的 60.9%;对于极早产儿和超早产儿,这一比例分别为 1.0%和 36.5%,0.4%和 20.0%。总体而言,母亲在分娩住院期间承担了总费用的 56%。
产妇和新生儿的费用都存在偏倚,而婴儿的偏倚更为明显。早产儿分娩比足月分娩昂贵得多,额外的费用主要由婴儿承担。需要在新生儿重症监护病房长期住院的婴儿比例很小,但却占新生儿费用的很大比例,而且这些费用随着时间的推移而增加。