Global Health Section, Department of Public Health, University of Copenhagen, Copenhagen, Denmark.
Department of Clinical Sciences, Lund University, Malmö, Sweden.
Int J Gynaecol Obstet. 2019 Jan;144(1):27-36. doi: 10.1002/ijgo.12692. Epub 2018 Oct 26.
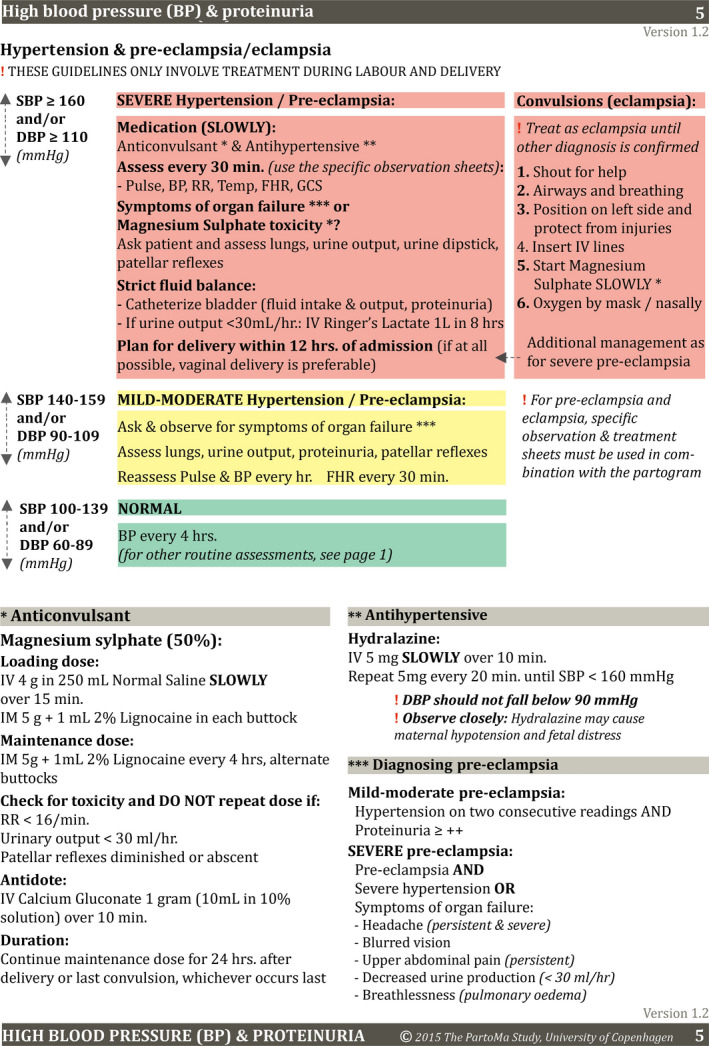
To estimate the effect of locally tailored clinical guidelines on intrapartum care and perinatal outcomes among women with severe hypertensive disorders in pregnancy (sHDP).
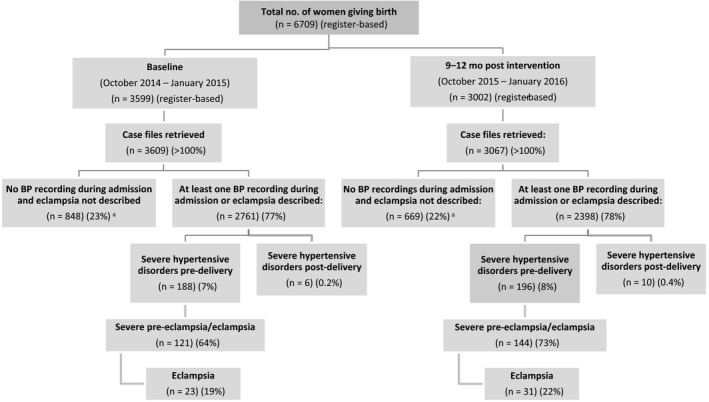
A pre-post study at Zanzibar's low-resource Mnazi Mmoja Hospital was conducted. All labouring women with sHDP were included at baseline (October 2014 to January 2015) and at 9-12 months after implementation of the ongoing intervention (October 2015 to January 2016). Background characteristics, clinical practice, and delivery outcomes were assessed by criterion-based case file reviews.
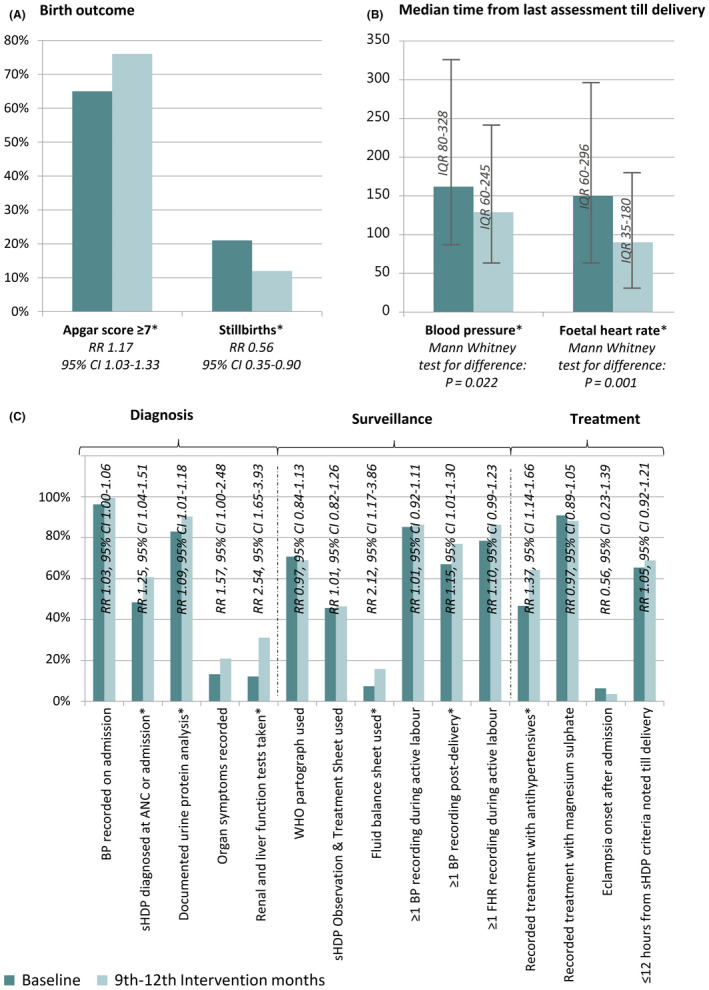
Overall, 188 of 2761 (6.8%) women had sHDP at baseline, and 196 of 2398 (8.2%) did so during the intervention months. The median time between last blood pressure recording and delivery decreased during the intervention compared with baseline (P=0.015). Among women with severe hypertension, antihypertensive treatment increased during the intervention compared with baseline (relative risk [RR] 1.37, 95% confidence interval [CI] 1.14-1.66). Among the neonates delivered (birthweight ≥1000 g), stillbirths decreased (RR 0.56, 95% CI 0.35-0.90) and Apgar scores of seven or more increased during the intervention compared with baseline (RR 1.17, 95% CI 1.03-1.33).
Although health system strengthening remains crucial, locally tailored clinical guidelines seemed to help work-overloaded birth attendants at a low-resource hospital to improve care for women with sHDP. CLINICALTRIALS.ORG: NCT02318420.
评估针对妊娠重度高血压疾病(sHDP)患者的个体化临床指南对产时护理和围产结局的影响。
在坦桑尼亚资源有限的 Mnazi Mmoja 医院进行了一项前后对照研究。所有患有 sHDP 的产妇均在基线期(2014 年 10 月至 2015 年 1 月)和正在进行的干预实施后 9-12 个月(2015 年 10 月至 2016 年 1 月)纳入研究。通过基于标准的病历回顾评估背景特征、临床实践和分娩结局。
总体而言,2761 例产妇中有 188 例(6.8%)在基线期患有 sHDP,2398 例中有 196 例(8.2%)在干预期患有 sHDP。与基线相比,干预期间最后一次血压记录与分娩之间的时间中位数缩短(P=0.015)。在患有严重高血压的产妇中,干预期间的降压治疗较基线增加(相对风险 [RR] 1.37,95%置信区间 [CI] 1.14-1.66)。在分娩的新生儿中(出生体重≥1000g),死胎减少(RR 0.56,95%CI 0.35-0.90),且干预期间 Apgar 评分≥7 分的新生儿比例增加(RR 1.17,95%CI 1.03-1.33)。
尽管卫生系统强化仍然至关重要,但个体化临床指南似乎有助于帮助资源有限的医院中工作负荷过重的分娩医护人员改善对 sHDP 患者的护理。临床试验注册:NCT02318420。