Oladapo O T, Adetoro O O, Ekele B A, Chama C, Etuk S J, Aboyeji A P, Onah H E, Abasiattai A M, Adamu A N, Adegbola O, Adeniran A S, Aimakhu C O, Akinsanya O, Aliyu L D, Ande A B, Ashimi A, Bwala M, Fabamwo A, Geidam A D, Ikechebelu J I, Imaralu J O, Kuti O, Nwachukwu D, Omo-Aghoja L, Tunau K, Tukur J, Umeora Ouj, Umezulike A C, Dada O A, Tunçalp Ӧ, Vogel J P, Gülmezoglu A M
Department of Reproductive Health and Research including UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP), World Health Organization, Geneva, Switzerland.
Department of Obstetrics and Gynaecology, Olabisi Onabanjo University Teaching Hospital, Sagamu, Nigeria.
BJOG. 2016 May;123(6):928-38. doi: 10.1111/1471-0528.13450. Epub 2015 May 14.
To investigate the burden and causes of life-threatening maternal complications and the quality of emergency obstetric care in Nigerian public tertiary hospitals.
Nationwide cross-sectional study.
Forty-two tertiary hospitals.
Women admitted for pregnancy, childbirth and puerperal complications.
All cases of severe maternal outcome (SMO: maternal near-miss or maternal death) were prospectively identified using the WHO criteria over a 1-year period.
Incidence and causes of SMO, health service events, case fatality rate, and mortality index (% of maternal death/SMO).
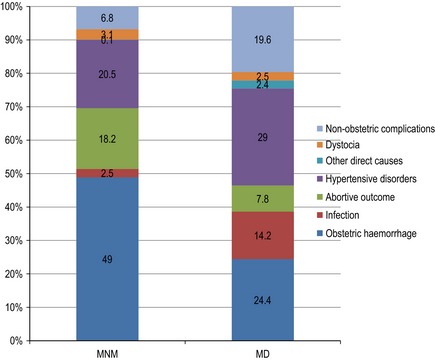
Participating hospitals recorded 91 724 live births and 5910 stillbirths. A total of 2449 women had an SMO, including 1451 near-misses and 998 maternal deaths (2.7, 1.6 and 1.1% of live births, respectively). The majority (91.8%) of SMO cases were admitted in critical condition. Leading causes of SMO were pre-eclampsia/eclampsia (23.4%) and postpartum haemorrhage (14.4%). The overall mortality index for life-threatening conditions was 40.8%. For all SMOs, the median time between diagnosis and critical intervention was 60 minutes (IQR: 21-215 minutes) but in 21.9% of cases, it was over 4 hours. Late presentation (35.3%), lack of health insurance (17.5%) and non-availability of blood/blood products (12.7%) were the most frequent problems associated with deficiencies in care.
Improving the chances of maternal survival would not only require timely application of life-saving interventions but also their safe, efficient and equitable use. Maternal mortality reduction strategies in Nigeria should address the deficiencies identified in tertiary hospital care and prioritise the prevention of severe complications at lower levels of care.
Of 998 maternal deaths and 1451 near-misses reported in a network of 42 Nigerian tertiary hospitals in 1 year.
调查尼日利亚公立三级医院危及生命的孕产妇并发症负担及原因,以及产科急诊护理质量。
全国性横断面研究。
42家三级医院。
因妊娠、分娩及产褥期并发症入院的女性。
采用世界卫生组织标准,前瞻性地识别1年内所有严重孕产妇结局(SMO:孕产妇接近死亡或孕产妇死亡)病例。
SMO的发生率及原因、卫生服务事件、病死率和死亡指数(孕产妇死亡数/SMO的百分比)。
参与研究的医院记录了91724例活产和5910例死产。共有2449名女性出现SMO,包括1451例接近死亡和998例孕产妇死亡(分别占活产数的2.7%、1.6%和1.1%)。大多数(91.8%)SMO病例入院时病情危急。SMO的主要原因是子痫前期/子痫(23.4%)和产后出血(14.4%)。危及生命情况的总体死亡指数为40.8%。对于所有SMO病例,诊断至关键干预的中位时间为60分钟(四分位间距:21 - 215分钟),但在21.9%的病例中,超过4小时。就诊延迟(35.3%)、缺乏医疗保险(17.5%)和血液/血制品供应不足(12.7%)是与护理缺陷相关的最常见问题。
提高孕产妇生存几率不仅需要及时应用挽救生命的干预措施,还需要安全、有效且公平地使用这些措施。尼日利亚的孕产妇死亡率降低策略应解决三级医院护理中发现的缺陷,并优先在较低护理级别预防严重并发症。
在尼日利亚42家三级医院网络中,1年报告了998例孕产妇死亡和1451例接近死亡病例。