Pikija Slaven, Trkulja Vladimir, Ramesmayer Christian, Mutzenbach Johannes S, Killer-Oberpfalzer Monika, Hecker Constantin, Bubel Nele, Füssel Michael Ulrich, Sellner Johann
Department of Neurology, Christian Doppler Medical Center, Paracelsus Medical University, Salzburg, Austria.
Department for Pharmacology, School of Medicine, University of Zagreb, Zagreb, Croatia.
J Stroke. 2018 Sep;20(3):373-384. doi: 10.5853/jos.2018.01305. Epub 2018 Sep 30.
Reports investigating the relationship between in-procedure blood pressure (BP) and outcomes in patients undergoing endovascular thrombectomy (EVT) due to anterior circulation stroke are sparse and contradictory.
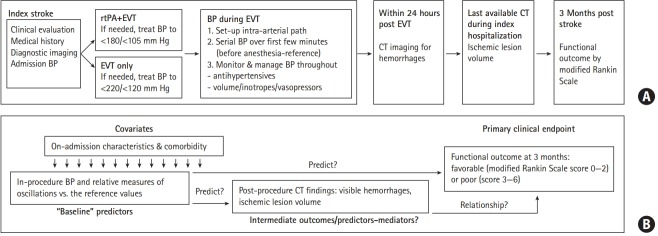
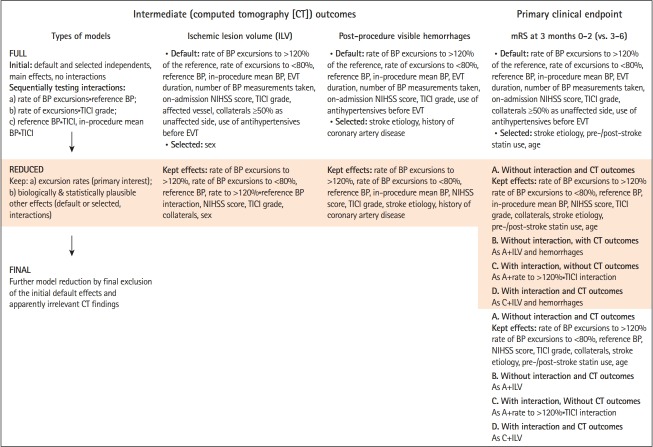
Consecutive EVT-treated adults (modern stent retrievers, BP managed in line with the recommendations, general anesthesia, invasive BP measurements) were evaluated for associations of the rate of in-procedure systolic BP (SBP) and mean arterial pressure (MAP) excursions to >120%/<80% of the reference values (serial measurements at anesthesia induction) and of the reference BP/weighted in-procedure mean BP with post-procedure imaging outcomes (ischemic lesion volume [ILV], hemorrhages) and 3-month functional outcome (modified Rankin Scale [mRS], score 0 to 2 vs. 3 to 6).
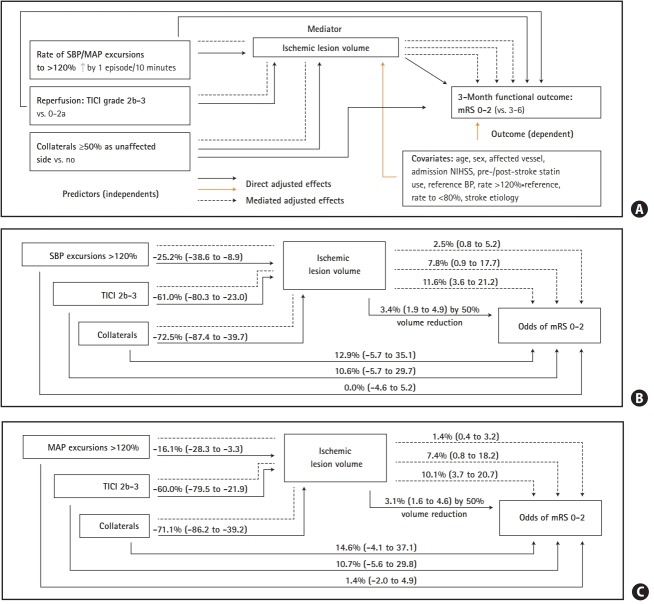
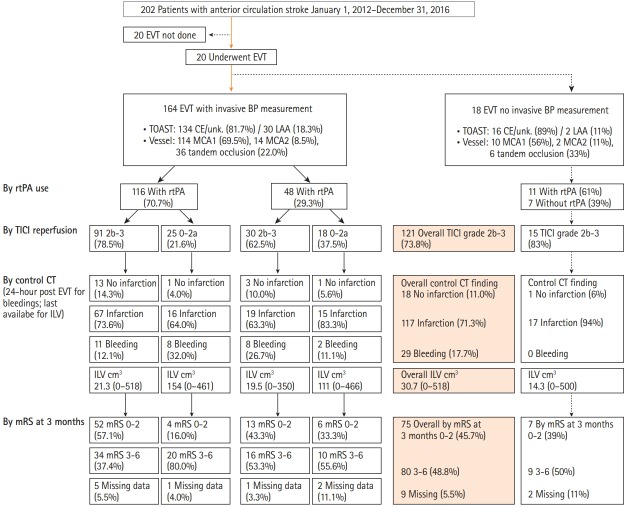
Overall 164 patients (70.7% pharmacological reperfusion, 80.5% with good collaterals, 73.8% with successful reperfusion) were evaluated for ILV (range, 0 to 581 cm3) and hemorrhages (incidence 17.7%). Higher rate of in-procedure SBP/MAP excursions to >120% was independently associated with lower ILV, while higher in-procedure mean SBP/MAP was associated with lower odds of hemorrhages. mRS 0-2 was achieved in 75/155 (48.4%) evaluated patients (nine had missing mRS data). Higher rate of SBP/MAP excursions to >120% and higher reference SBP/MAP were independently associated with higher odds of mRS 0-2, while higher ILV was associated with lower odds of mRS 0-2. Rate of SBP/MAP excursions to <80% was not associated with any outcome.
s In the EVT-treated patients with BP managed within the recommended limits, a better functional outcome might be achieved by targeting in-procedure BP that exceeds the preprocedure values by more than 20%.
关于血管内血栓切除术(EVT)治疗前循环卒中患者时,术中血压(BP)与预后关系的研究报告较为稀少且相互矛盾。
对连续接受EVT治疗的成年人(使用现代支架取栓器,按照推荐管理血压,全身麻醉,有创血压测量)进行评估,分析术中收缩压(SBP)和平均动脉压(MAP)超过参考值(麻醉诱导时的连续测量值)的120%/低于80%的发生率,以及参考血压/术中加权平均血压与术后影像学结果(缺血性病变体积[ILV]、出血情况)和3个月功能预后(改良Rankin量表[mRS],0至2分与3至6分)之间的关联。
共评估了164例患者(70.7%接受药物再灌注,80.5%侧支循环良好,73.8%再灌注成功)的ILV(范围为0至581 cm³)和出血情况(发生率为17.7%)。术中SBP/MAP超过120%的发生率较高与较低的ILV独立相关,而术中较高的平均SBP/MAP与较低的出血几率相关。在155例接受评估的患者中,75例(48.4%)达到了mRS 0 - 2(9例mRS数据缺失)。SBP/MAP超过120%的发生率较高以及较高的参考SBP/MAP与较高的mRS 0 - 2几率独立相关,而较高的ILV与较低的mRS 0 - 2几率相关。SBP/MAP低于80%的发生率与任何预后均无关联。
在血压控制在推荐范围内接受EVT治疗的患者中,将术中血压目标设定为超过术前值20%以上可能会获得更好的功能预后。