From the Departments of Radiology & Nuclear Medicine (N.S., R.A.v.d.G., C.A.L.v.d.B., B.R., A.v.d.L., A.C.G.M.v.E.), Public Health (D.N., H.F.L.), Anesthesiology (I.E.), and Neurology (N.S., R.A.v.d.G., B.R., D.W.J.D.), Erasmus MC, University Medical Center, Rotterdam; Departments of Radiology & Nuclear Medicine (K.M.T., B.J.E., C.B.L.M.M.) and Anesthesiology (R.V.I.), Amsterdam University Medical Center, University of Amsterdam; Department of Radiology and Nuclear Medicine, Cardiovascular Research Institute Maastricht (W.H.v.Z.), Maastricht University Medical Center; Departments of Radiology and Nuclear Medicine (R.P.H.B., M.U.) and Neurology (M.U.), University Medical Center Groningen; Department of Radiology and Nuclear Medicine (B.A.A.M.v.H.), Isala, Zwolle; Department of Anesthesiology, Pain & Palliative Medicine (J.M.), Radboud UMC, University Medical Center, Nijmegen, the Netherlands; and Department of Neurology (J.F.B.), University of Michigan, Ann Arbor.
Neurology. 2021 Jan 12;96(2):e171-e181. doi: 10.1212/WNL.0000000000011006. Epub 2020 Oct 7.
To evaluate the role of blood pressure (BP) as mediator of the effect of conscious sedation (CS) compared to local anesthesia (LA) on functional outcome after endovascular treatment (EVT).
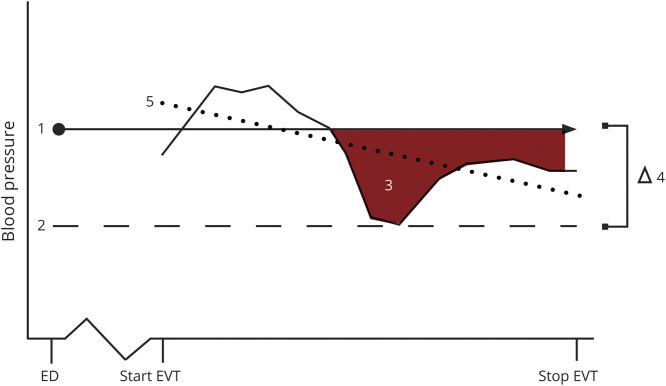
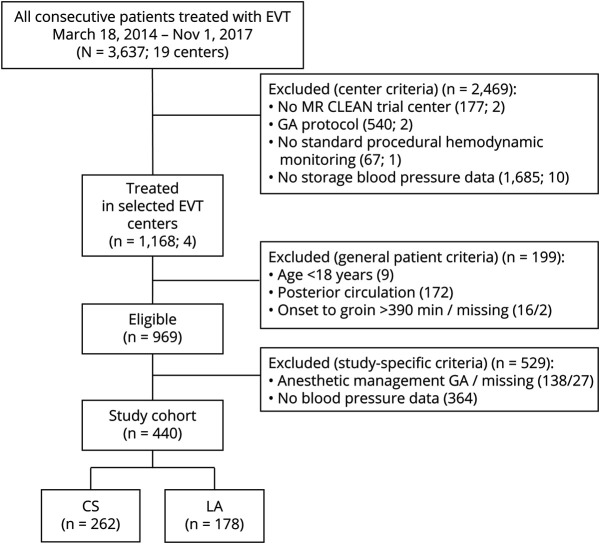
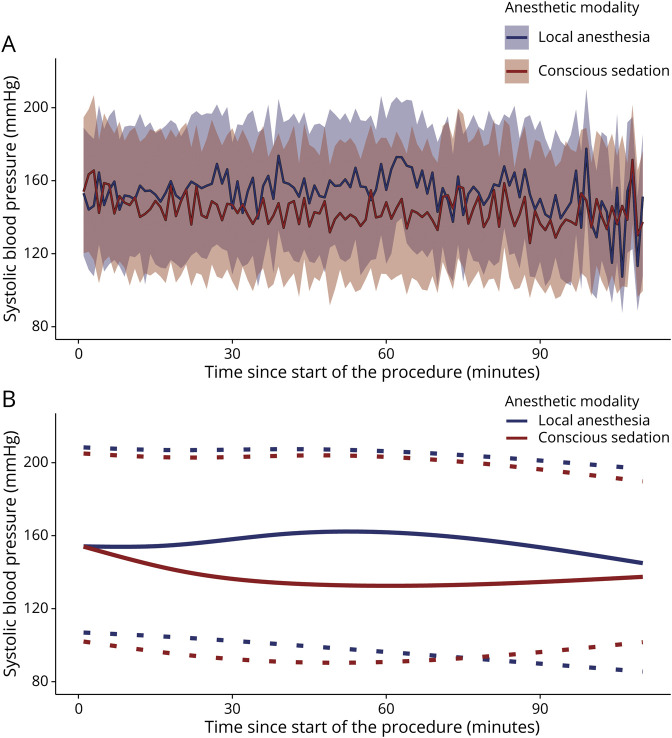
Patients treated in the Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN) Registry centers with CS or LA as preferred anesthetic approach during EVT for ischemic stroke were analyzed. First, we evaluated the effect of CS on area under the threshold (AUT), relative difference between baseline and lowest procedural mean arterial pressure (∆LMAP), and procedural BP trend, compared to LA. Second, we assessed the association between BP and functional outcome (modified Rankin Scale [mRS]) with multivariable regression. Lastly, we evaluated whether BP explained the effect of CS on mRS.
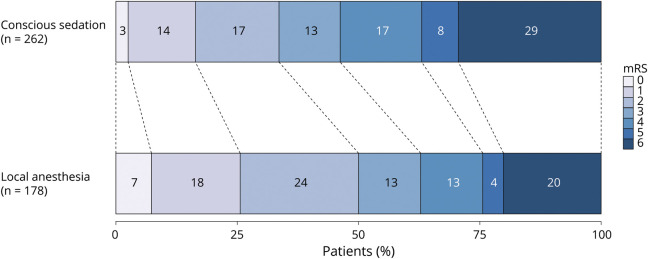
In 440 patients with available BP data, patients treated under CS (n = 262) had larger AUTs (median 228 vs 23 mm Hgmin), larger ∆LMAP (median 16% vs 6%), and a more negative BP trend (-0.22 vs -0.08 mm Hg/min) compared to LA (n = 178). Larger ∆LMAP and AUTs were associated with worse mRS (adjusted common odds ratio [acOR] per 10% drop 0.87, 95% confidence interval [CI] 0.78-0.97, and acOR per 300 mm Hgmin 0.89, 95% CI 0.82-0.97). Patients treated under CS had worse mRS compared to LA (acOR 0.59, 95% CI 0.40-0.87) and this association remained when adjusting for ∆LMAP and AUT (acOR 0.62, 95% CI 0.42-0.92).
Large BP drops are associated with worse functional outcome. However, BP drops do not explain the worse outcomes in the CS group.
评估血压(BP)作为意识镇静(CS)与局部麻醉(LA)对急性缺血性卒中血管内治疗(EVT)后功能结局影响的中介作用。
对在荷兰多中心急性缺血性卒中血管内治疗随机临床试验(MR CLEAN)登记中心接受 CS 或 LA 作为 EVT 期间首选麻醉方法治疗的患者进行分析。首先,我们评估了 CS 对阈下面积(AUT)、基线与最低程序平均动脉压(∆LMAP)之间的相对差值以及程序 BP 趋势的影响,与 LA 相比。其次,我们使用多变量回归评估了 BP 与功能结局(改良 Rankin 量表[mRS])之间的关联。最后,我们评估了 BP 是否解释了 CS 对 mRS 的影响。
在 440 例具有可用 BP 数据的患者中,接受 CS 治疗的患者(n = 262)AUT 更大(中位数 228 比 23mmHgmin),∆LMAP 更大(中位数 16%比 6%),BP 趋势更负(-0.22 比 -0.08mmHg/min),与 LA 治疗的患者(n = 178)相比。较大的 ∆LMAP 和 AUT 与更差的 mRS 相关(每下降 10%的调整后的常见优势比[aOR]为 0.87,95%置信区间[CI]为 0.78-0.97,每增加 300mmHgmin 的 aOR 为 0.89,95%CI 为 0.82-0.97)。与 LA 相比,接受 CS 治疗的患者 mRS 更差(aOR 0.59,95%CI 0.40-0.87),当调整 ∆LMAP 和 AUT 时,这种关联仍然存在(aOR 0.62,95%CI 0.42-0.92)。
大的 BP 下降与更差的功能结局相关。然而,BP 下降并不能解释 CS 组结局更差的原因。