Guner Yigit S, Harting Matthew T, Fairbairn Kelly, Delaplain Patrick T, Zhang Lishi, Chen Yanjun, Kabeer Mustafa H, Yu Peter, Cleary John P, Stein James E, Stolar Charles, Nguyen Danh V
Children's Hospital of Orange County, Division of Pediatric Surgery, Orange, CA; University of California Irvine Medical Center, Department of Surgery, Orange, CA.
Department of Pediatric Surgery, University of Texas McGovern Medical School and Children's Memorial Hermann Hospital, Houston, TX.
J Pediatr Surg. 2018 Nov;53(11):2092-2099. doi: 10.1016/j.jpedsurg.2018.06.003. Epub 2018 Jun 7.
Previous studies comparing extracorporeal membrane oxygenation (ECMO) modality for congenital diaphragmatic hernia (CDH) have not accounted for confounding by indication. We therefore hypothesized that using a propensity score (PS) approach to account for selection bias may identify outcome differences based on ECMO modality for infants with CDH.
We utilized ELSO Registry data (2000-2016). Patients with CDH were divided to either venoarterial (VA) or venovenous (VV) ECMO. Patients were matched by PS to control for nonrandom treatment assignment. Subgroup analyses were conducted based on timing of CDH repair relative to ECMO. Primary analysis was the "intent-to-treat" cohort based on the initial ECMO mode. Mortality was the primary outcome, and severe neurologic injury (SNI) was a secondary outcome.
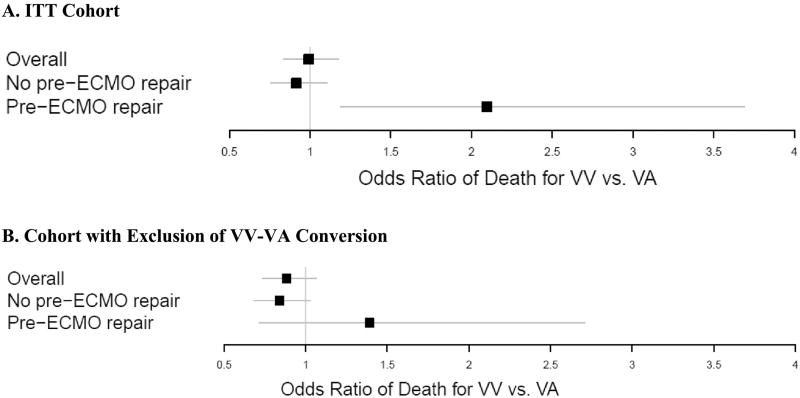
PS matching (3:1) identified 3304 infants (VA = 2470, VV = 834). In the main group, mortality was not different between VA and VV ECMO (OR = 1.01, 95% CI: 0.86-1.18) and there was no difference in SNI between VA and VV (OR = 0.80; 95% CI: 0.63-1.01). For the pre-ECMO CDH repair subgroup, 175 VA cases were matched to 70 VV. In these neonates, mortality was higher for VV compared to VA (OR = 2.10, 95% CI: 1.19-3.69), without any difference in SNI (OR = 1.48; 95% CI: 0.59-3.71). For the subgroup that did not have pre-ECMO CDH repair, 2030 VA cases were matched to 683 VV cases. In this subgroup, VV was associated with 27% lower risk of SNI relative to VA (OR = 0.73, 95% CI: 0.56-0.95) without any difference in mortality (OR = 0.94, 95% CI: 0.79-1.11).
This study revalidates that ECMO mode does not significantly affect mortality or SNI in infants with CDH. In the subset of infants who require pre-ECMO CDH repair, VA favors survival, whereas, in the subgroup of infants that did not have pre-ECMO CDH repair, VV favors lower rates of SNI. We conclude that neither mode appears consistently superior across all situations, and clinical judgment should remain a multifactorial decision.
Level III.
既往比较先天性膈疝(CDH)体外膜肺氧合(ECMO)模式的研究未考虑适应证的混杂因素。因此,我们假设采用倾向评分(PS)方法来解释选择偏倚,可能会发现基于ECMO模式的CDH婴儿结局差异。
我们利用体外生命支持组织(ELSO)注册数据(2000 - 2016年)。将CDH患者分为静脉 - 动脉(VA)或静脉 - 静脉(VV)ECMO组。通过PS对患者进行匹配,以控制非随机治疗分配。根据CDH修复相对于ECMO的时间进行亚组分析。主要分析是基于初始ECMO模式的“意向性治疗”队列。死亡率是主要结局,严重神经损伤(SNI)是次要结局。
PS匹配(3:1)确定了3304例婴儿(VA = 2470例,VV = 834例)。在主要组中,VA和VV ECMO的死亡率无差异(OR = 1.01,95%CI:0.86 - 1.18),VA和VV的SNI也无差异(OR = 0.80;95%CI:0.63 - 1.01)。对于ECMO前CDH修复亚组,175例VA病例与70例VV病例匹配。在这些新生儿中,VV的死亡率高于VA(OR = 2.10,95%CI:1.19 - 3.69),SNI无差异(OR = 1.48;95%CI:0.59 - 3.71)。对于未进行ECMO前CDH修复的亚组,2030例VA病例与683例VV病例匹配。在该亚组中,相对于VA,VV的SNI风险降低27%(OR = 0.73,95%CI:0.56 - 0.95),死亡率无差异(OR = 0.94,95%CI:0.79 - 1.11)。
本研究再次验证ECMO模式对CDH婴儿的死亡率或SNI无显著影响。在需要ECMO前CDH修复的婴儿亚组中,VA有利于生存,而在未进行ECMO前CDH修复的婴儿亚组中,VV有利于降低SNI发生率。我们得出结论,在所有情况下,两种模式都没有始终表现出明显优势,临床判断应仍然是一个多因素的决策。
三级。