Ifakara Health Institute, Dar es Salaam, Tanzania.
National Institute for Medical Research, Tanga Research Centre, Tanga, Tanzania.
Malar J. 2018 Oct 17;17(1):369. doi: 10.1186/s12936-018-2524-x.
Artemisinin-based combination therapy (ACT) is the first-line anti-malarial treatment of uncomplicated malaria in most malaria endemic countries, including Tanzania. Unfortunately, there have been reports of artemisinin resistance and ACT failure from South East Asia highlighting the need to monitor therapeutic efficacy of ACT in these countries as recommended by World Health Organization.
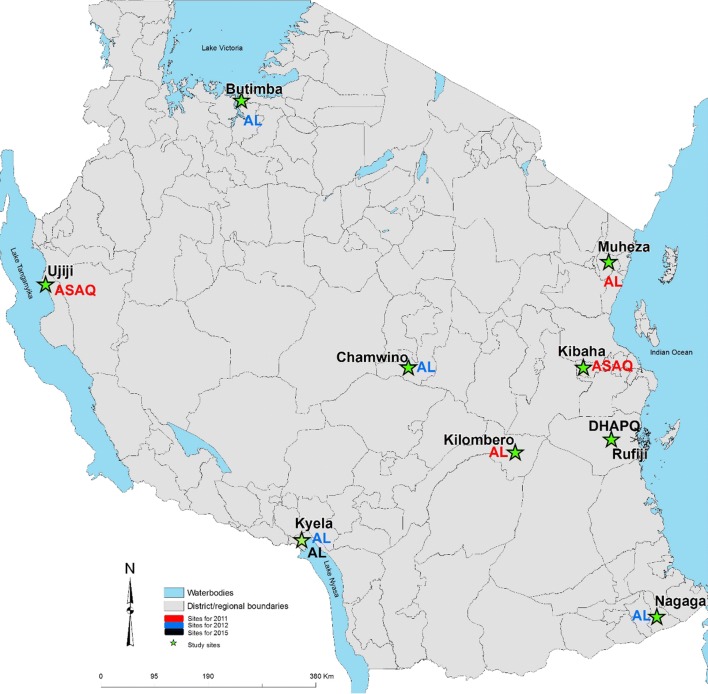
Open-label single arm studies in mainland Tanzania were conducted in nine sentinel sites in 2011, 2012 and 2015 to assess the efficacy and safety of artemether/lumefantrine (AL) and artesunate/amodiaquine (ASAQ) using 28 days follow-up and dihydroartemisinin/piperaquine (DHAPQ) using 42 days follow-up. Mutations in the propeller domain of the Plasmodium falciparum kelch 13 (k13) gene and amplification of the P. falciparum plasmepsin 2 (pm2) gene, associated with artemisinin and piperaquine (PQ) resistance, were also investigated.
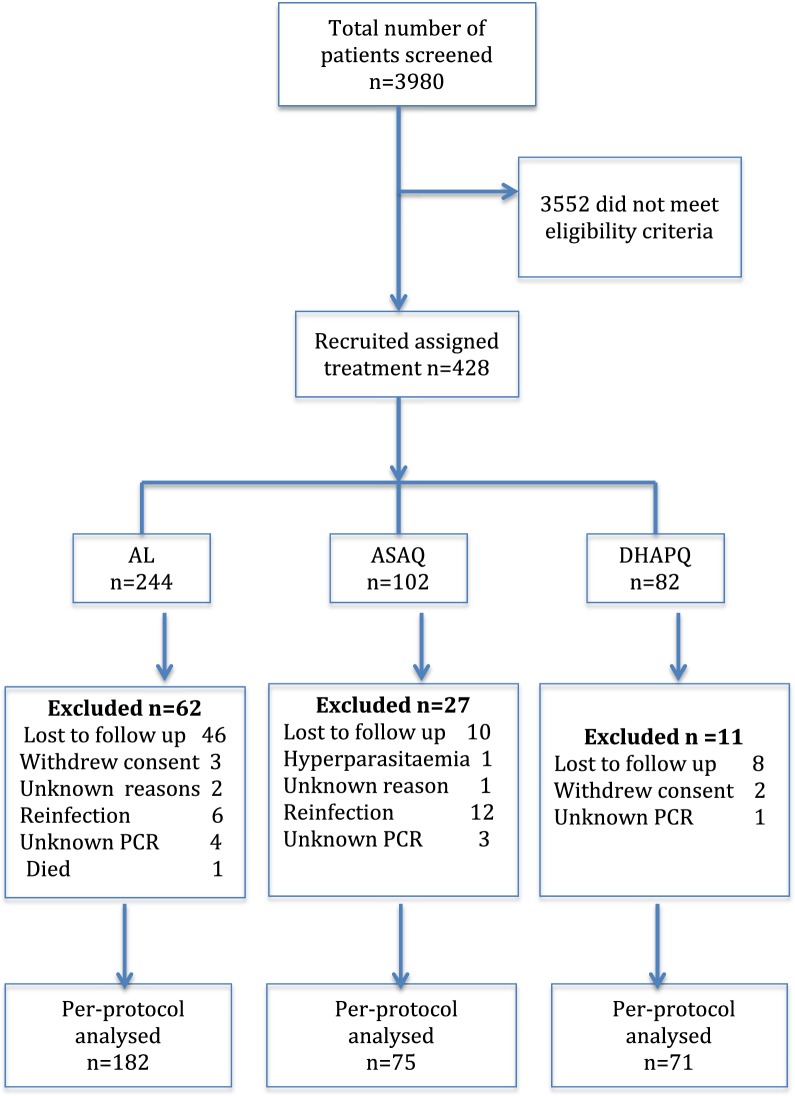
Of the 428 patients enrolled, 328 patients provided study endpoint. For AL, the PCR corrected per-protocol analysis showed adequate clinical and parasitological response (ACPR) of 90.3% (n = 28; 95% CI 74.2-98.0) in Kyela 2012, 95.7% (n = 22; 95% CI 78.1-99.0) in Chamwino, 100% in Muheza (n = 29; 95% CI 88.1-100), 100% in Nagaga (n = 39; 95% CI 91.0-100) and Kyela 2015 (n = 60; 95% CI 94.0-100). For ASAQ, PCR corrected ACPR of 98% (n = 49; 95% CI 89.4-99.9) and 100% (n = 25; 95% CI 86.3-100) were observed in 2011 in Ujiji and Kibaha, respectively. For DHAPQ, the ACPR was 100% (n = 71; 95% CI 94.9-100). Of the 235 samples with genetic interpretable results, only 7 (3%) had non-synonymous k13 mutations. None of these are candidate or validated markers of artemisinin resistance and all patients carrying these alleles cleared the parasites on day 3. Of the DHAPQ group, 10% (3/29) of the samples with interpretable results had pm2 multiple copies and none of them was associated with treatment failure.
All the tested ACT in mainland Tanzania were highly efficacious and none of validated k13 mutants associated with artemisinin resistance was observed. However, three isolates with multiple copy numbers of pm2 gene associated with PQ resistance among the limited samples tested successfully calls for further investigation. Trial registration Number ACTRN12615000159550. Registered 18th February 2015, https://www.anzctr.org.au/trial/MyTrial.aspx.
青蒿素类复方疗法(ACT)是包括坦桑尼亚在内的大多数疟疾流行国家治疗无并发症疟疾的一线抗疟药物。不幸的是,东南亚已经有青蒿素耐药和 ACT 失败的报告,这突显了世界卫生组织建议监测这些国家 ACT 的治疗效果的必要性。
2011 年、2012 年和 2015 年在坦桑尼亚大陆的 9 个哨点进行了开放性单臂研究,以评估青蒿琥酯/咯萘啶(AL)和青蒿琥酯/阿莫地喹(ASAQ)的疗效和安全性,采用 28 天随访,二氢青蒿素/哌喹(DHAPQ)采用 42 天随访。还调查了与青蒿素和哌喹(PQ)耐药相关的疟原虫kelch 13(k13)基因螺旋桨结构域的突变和疟原虫质体朊酶 2(pm2)基因的扩增。
428 名入组患者中,328 名患者提供了研究终点。对于 AL,PCR 校正后的方案分析显示,在 Kyela 2012 有 90.3%(n=28;95% CI 74.2-98.0)、Chamwino 有 95.7%(n=22;95% CI 78.1-99.0)、Muheza 有 100%(n=29;95% CI 88.1-100)、Nagaga 有 100%(n=39;95% CI 91.0-100)和 Kyela 2015 有 100%(n=60;95% CI 94.0-100)的 PCR 校正后的临床和寄生虫学缓解(ACPR)。对于 ASAQ,在 2011 年,Ujiji 和 Kibaha 分别观察到 98%(n=49;95% CI 89.4-99.9)和 100%(n=25;95% CI 86.3-100)的 PCR 校正 ACPR。对于 DHAPQ,ACPR 为 100%(n=71;95% CI 94.9-100)。在 235 个具有遗传可解释结果的样本中,只有 7 个(3%)具有非同义 k13 突变。这些突变均不是青蒿素耐药的候选或验证性标志物,所有携带这些等位基因的患者在第 3 天清除了寄生虫。在 DHAPQ 组中,10%(n=3/29)具有可解释结果的样本中 pm2 基因有多个拷贝,它们均与治疗失败无关。
在坦桑尼亚大陆,所有测试的 ACT 均具有高度疗效,且未观察到与青蒿素耐药相关的经验证的 k13 突变体。然而,在所测试的有限样本中,有三个分离株具有与 PQ 耐药相关的 pm2 基因的多个拷贝,这成功地引起了进一步的研究。试验注册号 ACTRN12615000159550。于 2015 年 2 月 18 日注册,https://www.anzctr.org.au/trial/MyTrial.aspx。