Tolentino Julio C, Schmidt Sergio L
Department of Neurology, Federal University of the State of Rio de Janeiro, Rio de Janeiro, Brazil.
Front Psychiatry. 2018 Oct 2;9:450. doi: 10.3389/fpsyt.2018.00450. eCollection 2018.
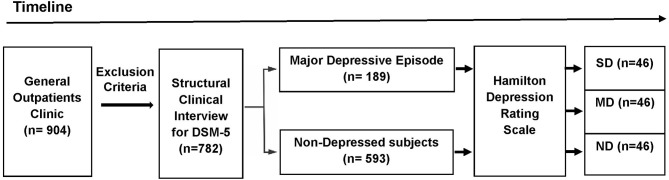
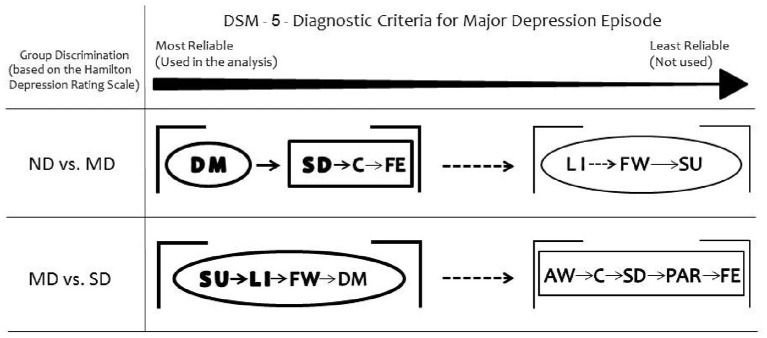
Depression diagnosis requires five or more symptoms (Diagnostic and Statistical Manual of Mental Disorders-DSM-5). One of them must be either Depressed mood or Anhedonia, named main criteria. Although the secondary symptoms can be divided into somatic and non-somatic clusters, the DSM-5 identify depression in all or none fashion. In contrast, depression severity is a continuous variable. Therefore, it is commonly assessed with scales such as the Hamilton Depression Rating Scale (HAMD). Previously, we reported that patients with moderate depression (MD) exhibit greater impairments in cardiac-autonomic modulation than severely depressed (SD) patients. However, clinicians usually do not use scales. To verify whether the DSM-5 symptoms would be able to discriminate SD from MD and MD from non-depressed (ND) subjects. Depression was diagnosed based on the Structured Clinical Interview for DSM-5® Disorders. The HAMD evaluated depression severity. In depressed subjects, MD and SD were defined considering the HAMD scores. ND was defined considering both the absence of DSM-5 criteria for depression and the HAMD score. Among 782 outpatients, 46 SD were found. MD and ND subjects were randomly sampled to match the demographic variables of the SD group. Discriminant analysis showed that Depressed Mood was the most reliable symptom to discriminate ND from MD. Anhedonia discriminated SD from MD. Among the secondary DSM-5 criteria, the somatic cluster discriminated ND from MD and the non-somatic cluster SD from MD patients. The presence of the somatic cluster in MD may indicate decreased vagal tone and/or increased sympathetic tone, leading to higher cardiovascular risk. As SD is associated with the non-somatic cluster, these patients are at risk of committing suicide. The DSM-5 symptoms exhibited by the patient may help the choice of adequate pharmacological treatment. This would avoid the use of antidepressants that unnecessarily increase cardiac risk in MD. When the symptom cluster suggests SD, the treatment must focus on the prevention of suicide. Depression severity may be inferred based on the DSM-5 criteria. The presence of the Anhedonia main criterium accompanied by non-somatic criteria indicate SD. The Depressive Mood criterium followed by somatic criteria suggest MD.
抑郁症的诊断需要出现五种或更多症状(《精神疾病诊断与统计手册》第五版 - DSM - 5)。其中之一必须是情绪低落或快感缺失,这被称为主要标准。虽然次要症状可分为躯体和非躯体两类,但DSM - 5以全有或全无的方式来认定抑郁症。相比之下,抑郁严重程度是一个连续变量。因此,通常使用如汉密尔顿抑郁评定量表(HAMD)等量表来评估。此前,我们报告中度抑郁症(MD)患者在心脏自主神经调节方面的损伤比重度抑郁症(SD)患者更大。然而,临床医生通常不使用量表。为了验证DSM - 5症状是否能够区分SD与MD以及MD与非抑郁症(ND)受试者。根据《DSM - 5® 障碍的结构化临床访谈》来诊断抑郁症。用HAMD评估抑郁严重程度。在抑郁症患者中,根据HAMD评分来定义MD和SD。ND的定义则既考虑不存在DSM - 5抑郁症标准,又考虑HAMD评分。在782名门诊患者中,发现46例SD患者。随机抽取MD和ND受试者以匹配SD组的人口统计学变量。判别分析表明,情绪低落是区分ND与MD最可靠的症状。快感缺失可区分SD与MD。在DSM - 5次要标准中,躯体类症状可区分ND与MD,非躯体类症状可区分SD与MD患者。MD患者中存在躯体类症状可能表明迷走神经张力降低和/或交感神经张力增加,导致心血管风险升高。由于SD与非躯体类症状相关,这些患者有自杀风险。患者表现出的DSM - 5症状可能有助于选择合适的药物治疗。这将避免使用不必要增加MD患者心脏风险的抗抑郁药。当症状群提示为SD时,治疗必须侧重于预防自杀。可根据DSM - 5标准推断抑郁严重程度。存在快感缺失主要标准并伴有非躯体类标准表明为SD。情绪低落标准之后伴有躯体类标准提示为MD。