Rensselaer Polytechnic Institute, 110, 8th Street, Troy, NY, 12180, USA.
University at Buffalo School of Medicine and Biomedical Sciences, Buffalo, NY, 14228, USA.
Surg Endosc. 2019 Aug;33(8):2485-2494. doi: 10.1007/s00464-018-6535-z. Epub 2018 Oct 17.
Physical and virtual surgical simulators are increasingly being used in training technical surgical skills. However, metrics such as completion time or subjective performance checklists often show poor correlation to transfer of skills into clinical settings. We hypothesize that non-invasive brain imaging can objectively differentiate and classify surgical skill transfer, with higher accuracy than established metrics, for subjects based on motor skill levels.
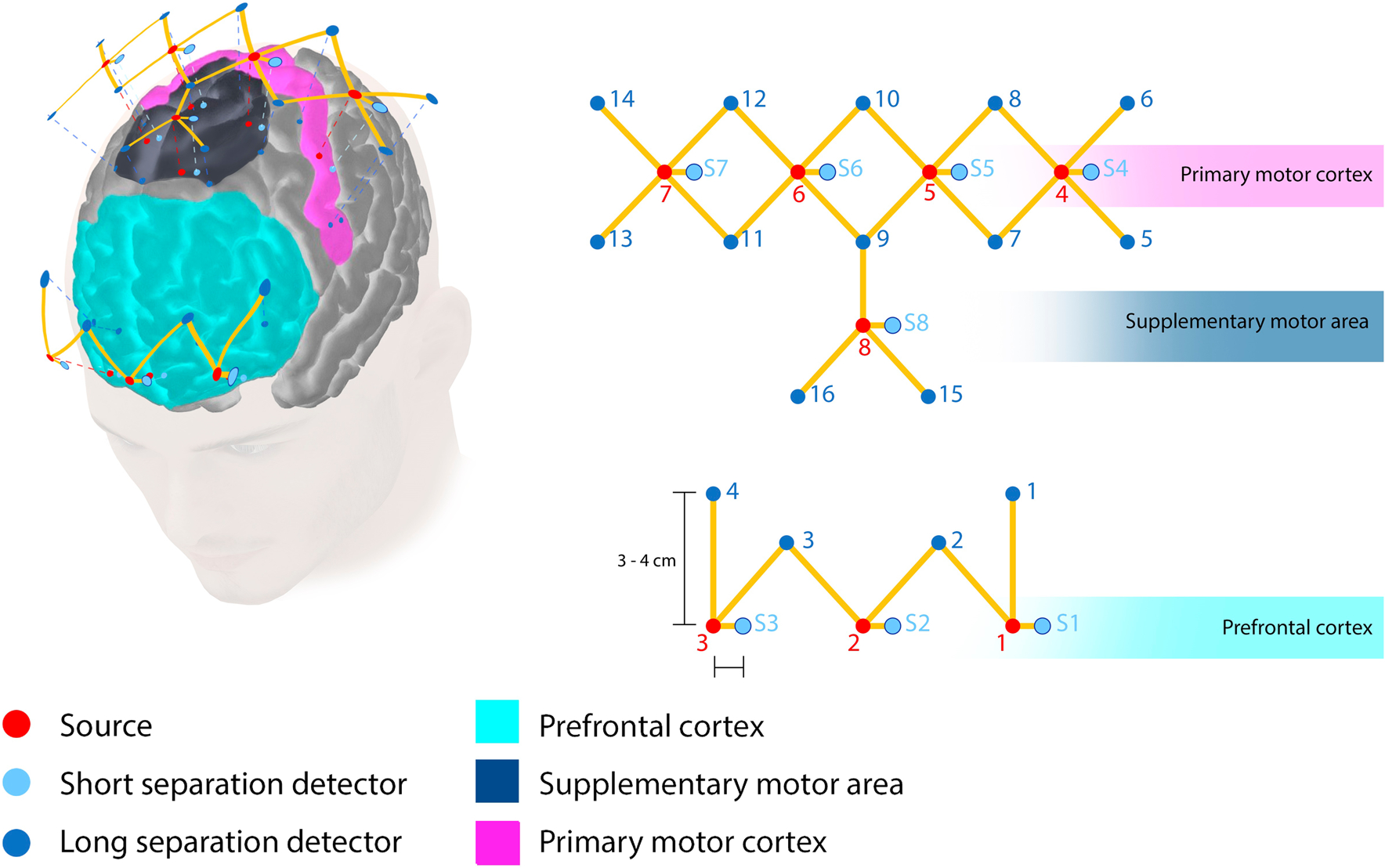
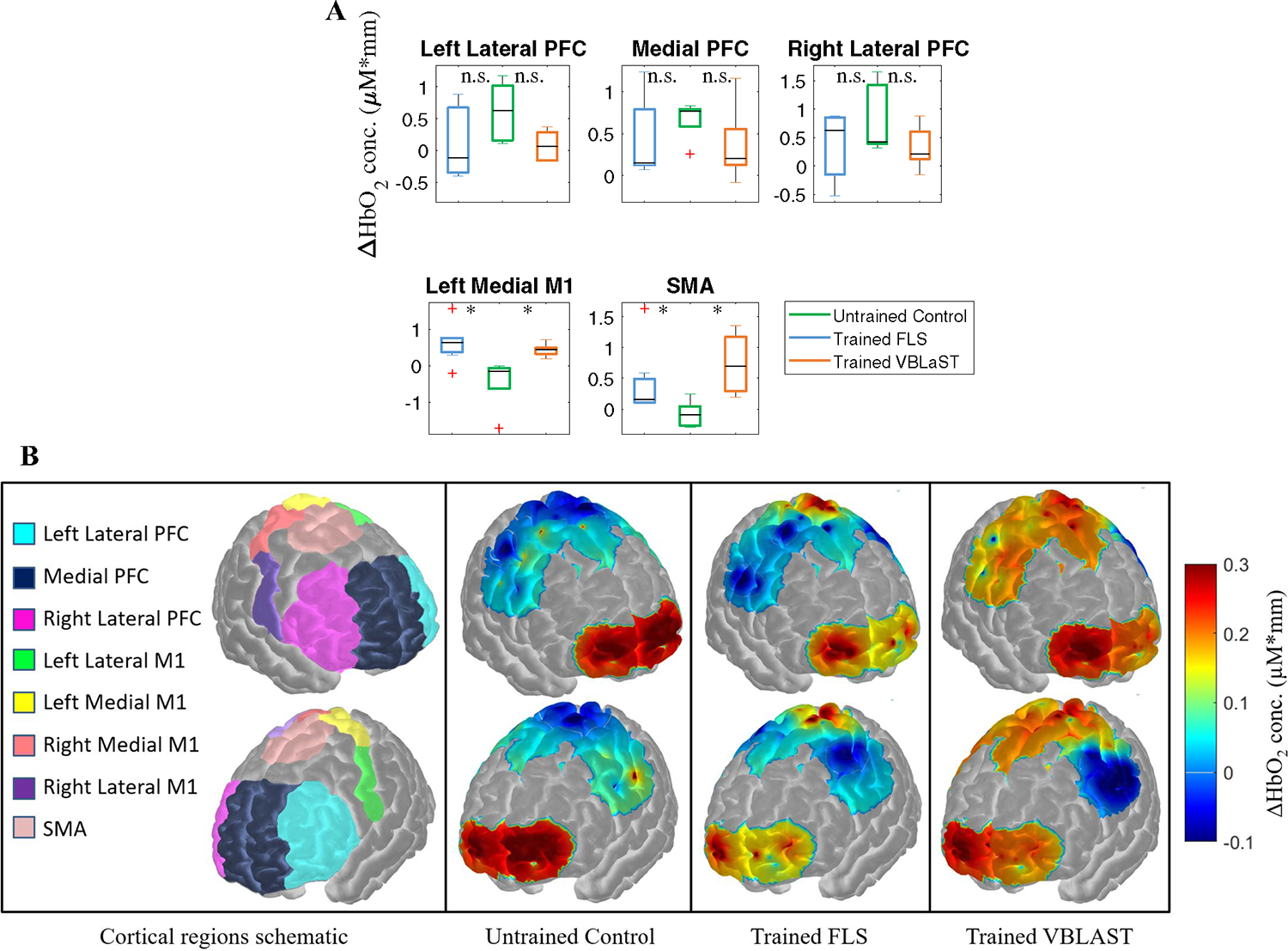
18 medical students at University at Buffalo were randomly assigned into control, physical surgical trainer, or virtual trainer groups. Training groups practiced a surgical technical task on respective simulators for 12 consecutive days. To measure skill transfer post-training, all subjects performed the technical task in an ex-vivo environment. Cortical activation was measured using functional near-infrared spectroscopy (fNIRS) in the prefrontal cortex, primary motor cortex, and supplementary motor area, due to their direct impact on motor skill learning.
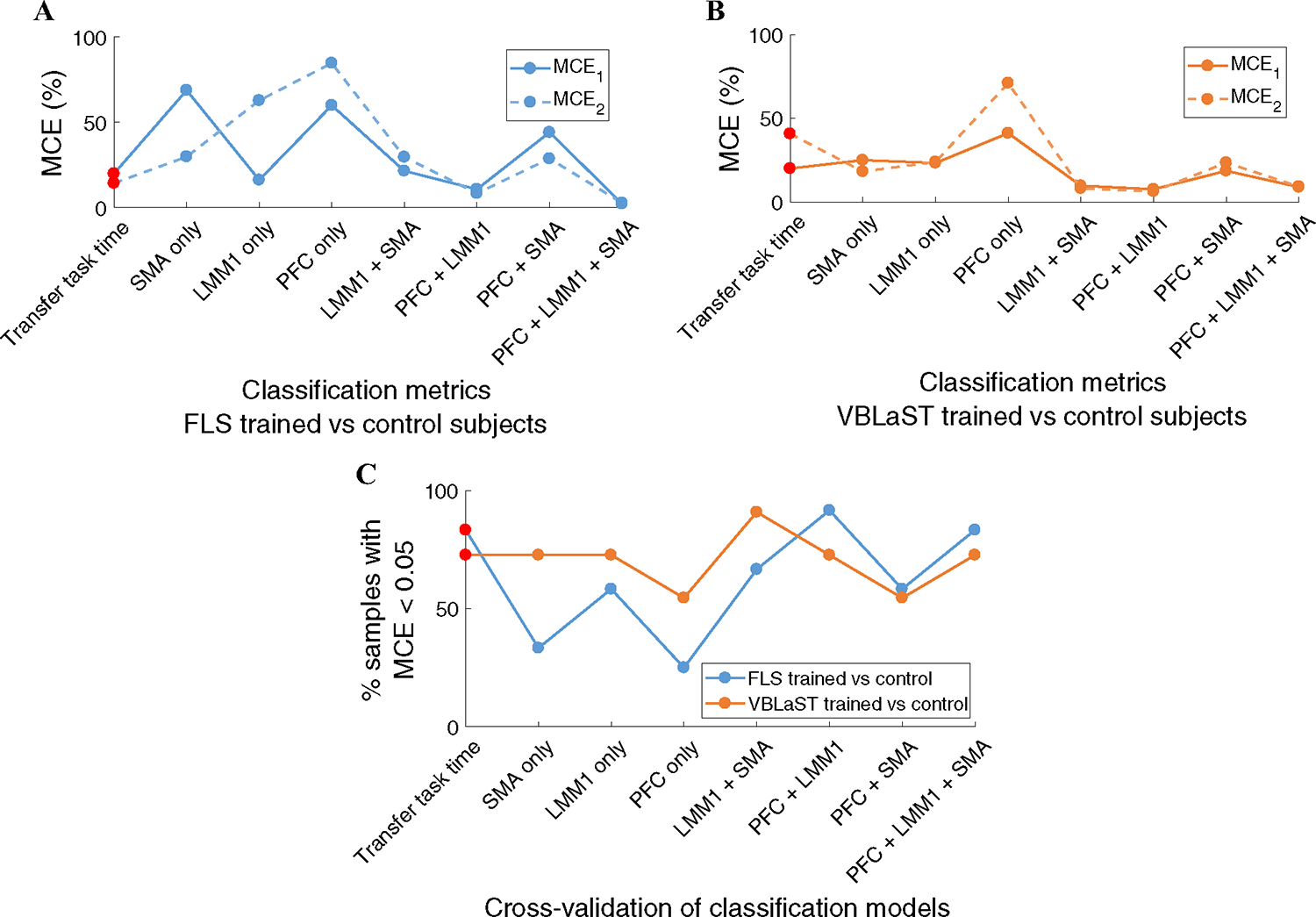
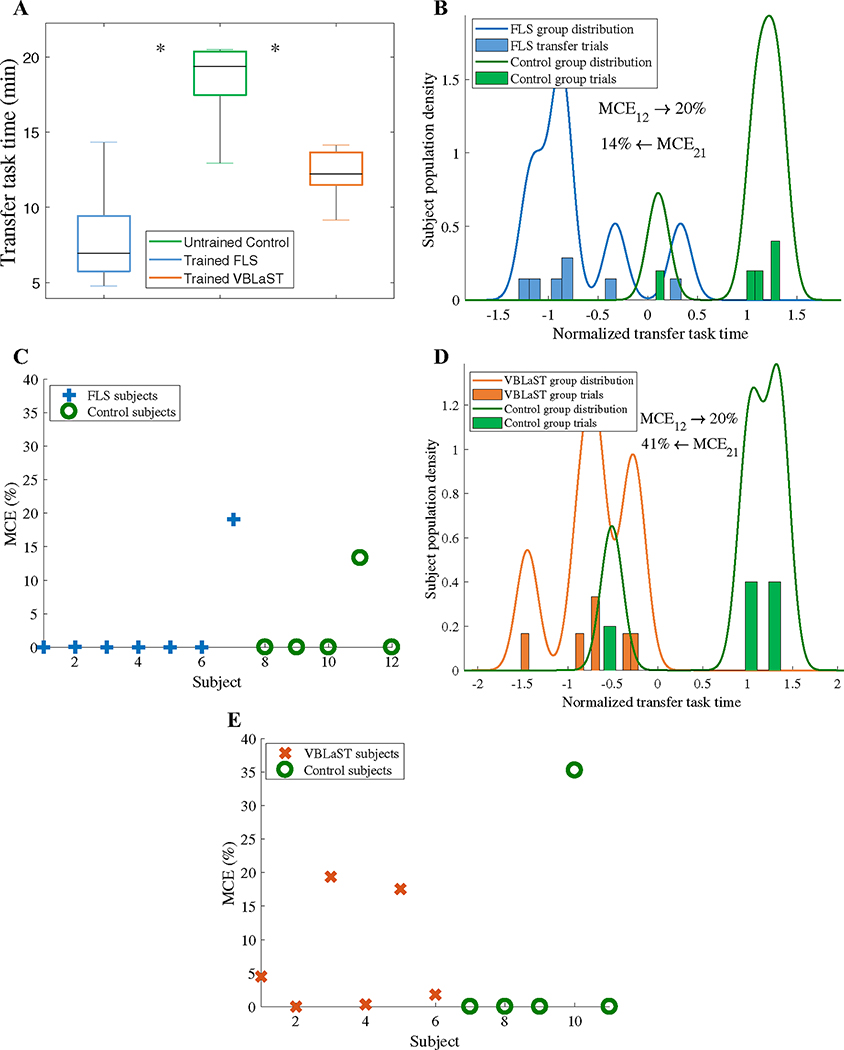
Classification between simulator trained and untrained subjects based on traditional metrics is poor, where misclassification errors range from 20 to 41%. Conversely, fNIRS metrics can successfully classify physical or virtual trained subjects from untrained subjects with misclassification errors of 2.2% and 8.9%, respectively. More importantly, untrained subjects are successfully classified from physical or virtual simulator trained subjects with misclassification errors of 2.7% and 9.1%, respectively.
fNIRS metrics are significantly more accurate than current established metrics in classifying different levels of surgical motor skill transfer. Our approach brings robustness, objectivity, and accuracy in validating the effectiveness of future surgical trainers in translating surgical skills to clinically relevant environments.
物理和虚拟手术模拟器越来越多地被用于培训技术手术技能。然而,完成时间或主观绩效检查表等指标通常与技能转移到临床环境的相关性较差。我们假设,无创脑成像可以客观地区分和分类手术技能转移,与传统指标相比,具有更高的准确性,基于运动技能水平对受试者进行分类。
18 名布法罗大学的医学生被随机分配到对照组、物理手术训练器组或虚拟训练器组。训练组在各自的模拟器上连续练习手术技术任务 12 天。为了测量培训后的技能转移,所有受试者在体外环境中执行该技术任务。使用功能近红外光谱(fNIRS)测量前额叶皮质、初级运动皮质和辅助运动区的皮质激活,因为它们直接影响运动技能学习。
基于传统指标对模拟器训练和未训练受试者进行分类的准确率较差,误分类错误率范围为 20%至 41%。相比之下,fNIRS 指标可以成功地将物理或虚拟训练的受试者与未训练的受试者进行分类,误分类错误率分别为 2.2%和 8.9%。更重要的是,未训练的受试者可以成功地从物理或虚拟模拟器训练的受试者中进行分类,误分类错误率分别为 2.7%和 9.1%。
fNIRS 指标在分类不同水平的手术运动技能转移方面明显比当前的既定指标更准确。我们的方法在验证未来手术训练器将手术技能转化为临床相关环境的有效性方面具有稳健性、客观性和准确性。