Daniel K Inouye College of Pharmacy, University of Hawai`i at Hilo, Hilo, USA
Daniel K Inouye College of Pharmacy, University of Hawai`i at Hilo, Hilo, USA.
BMJ Qual Saf. 2019 Feb;28(2):103-110. doi: 10.1136/bmjqs-2018-008418. Epub 2018 Oct 18.
We previously reported reduction in the rate of hospitalisations with medication harm among older adults with our 'Pharm2Pharm' intervention, a pharmacist-led care transition and care coordination model focused on best practices in medication management. The objectives of the current study are to determine the extent to which medication harm among older inpatients is 'community acquired' versus 'hospital acquired' and to assess the effectiveness of the Pharm2Pharm model with each type.
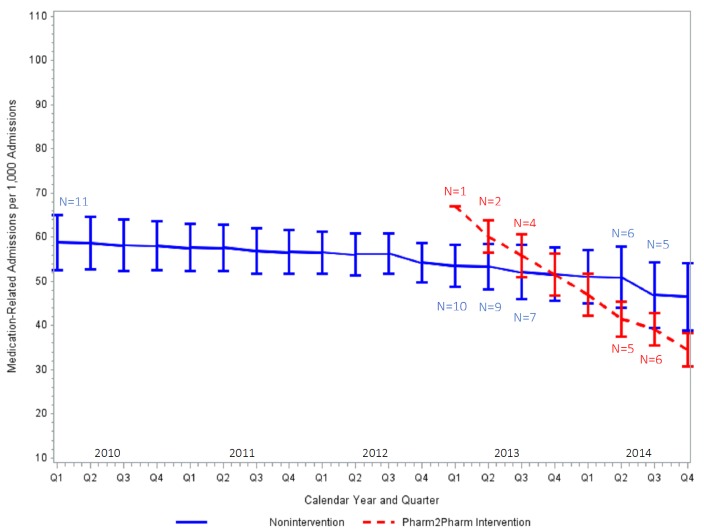
After a 3-year baseline, six non-federal general acute care hospitals with 50 or more beds in Hawaii implemented Pharm2Pharm sequentially. The other five such hospitals served as the comparison group. We measured frequencies and quarterly rates of admissions among those aged 65 and older with 'community-acquired' (International Classification of Diseases-coded as present on admission) and 'hospital-acquired' (coded as not present on admission) medication harm per 1000 admissions from 2010 to 2014.
There were 189 078 total admissions from 2010 through 2014, 7% of which had one or more medication harm codes. There were 16 225 medication harm codes, 70% of which were community-acquired, among these 13 795 admissions. The varied times when the intervention was implemented across hospitals were associated with a significant reduction in the rate of admissions with community-acquired medication harm compared with non-intervention hospitals (p=0.001), and specifically harm by anticoagulants (p<0.0001) and by medications in therapeutic use (p<0.001). The hospital-acquired medication harm rate did not change. The rate of admissions with community-acquired medication harm was reduced by 4.28 admissions per 1000 admissions per quarter in the Pharm2Pharm hospitals relative to the comparison hospitals.
The Pharm2Pharm model is an effective way to address the growing problem of community-acquired medication harm among high-risk, chronically ill patients. This model demonstrates the importance of deploying specially trained pharmacists in the hospital and in the community to systematically identify and resolve drug therapy problems.
我们之前报告了“Pharm2Pharm”干预措施可降低老年患者药物相关住院率,该措施是一种药师主导的医疗过渡和护理协调模式,专注于药物管理的最佳实践。本研究的目的是确定老年住院患者的药物相关伤害中有多大比例是“社区获得性”的,有多大比例是“医院获得性”的,并评估 Pharm2Pharm 模式对每种类型的有效性。
在 3 年基线后,夏威夷的六家非联邦综合急性护理医院先后实施了 Pharm2Pharm。其他五家类似的医院作为对照组。我们测量了 2010 年至 2014 年期间,年龄在 65 岁及以上的患者中每 1000 例入院因“社区获得性”(国际疾病分类编码为入院时存在)和“医院获得性”(编码为入院时不存在)药物相关伤害的频率和每季度发生率。
2010 年至 2014 年共有 189078 例总入院,其中 7%有一个或多个药物相关伤害编码。在这些 13795 例入院中,有 16225 个药物相关伤害编码,其中 70%是社区获得性的。由于干预措施在不同医院实施的时间不同,与非干预医院相比,社区获得性药物相关伤害入院率显著降低(p=0.001),特别是抗凝药物(p<0.0001)和治疗性药物(p<0.001)。医院获得性药物相关伤害率没有变化。Pharm2Pharm 医院每 1000 例入院每季度因社区获得性药物相关伤害而减少住院的人数为 4.28 人。
Pharm2Pharm 模式是解决高风险慢性病患者日益严重的社区获得性药物相关伤害问题的有效方法。该模式表明,在医院和社区部署经过专门培训的药剂师来系统地识别和解决药物治疗问题非常重要。