Azienda Ospedaliera Universitaria Federico II, Naples, Italy.
National Research Council, Institute of Biostructures and Bioimaging, Naples, Italy.
Radiat Oncol. 2018 Oct 19;13(1):202. doi: 10.1186/s13014-018-1146-3.
Technological advances in Hodgkin lymphoma (HL) radiation therapy (RT) by high conformal treatments potentially increase control over organs-at-risk (OARs) dose distribution. However, plan optimization remains a time-consuming task with great operator dependent variability. Purpose of the present study was to devise a fully automated pipeline based on the Pinnacle Auto-Planning (AP) algorithm for treating female supradiaphragmatic HL (SHL) patients.
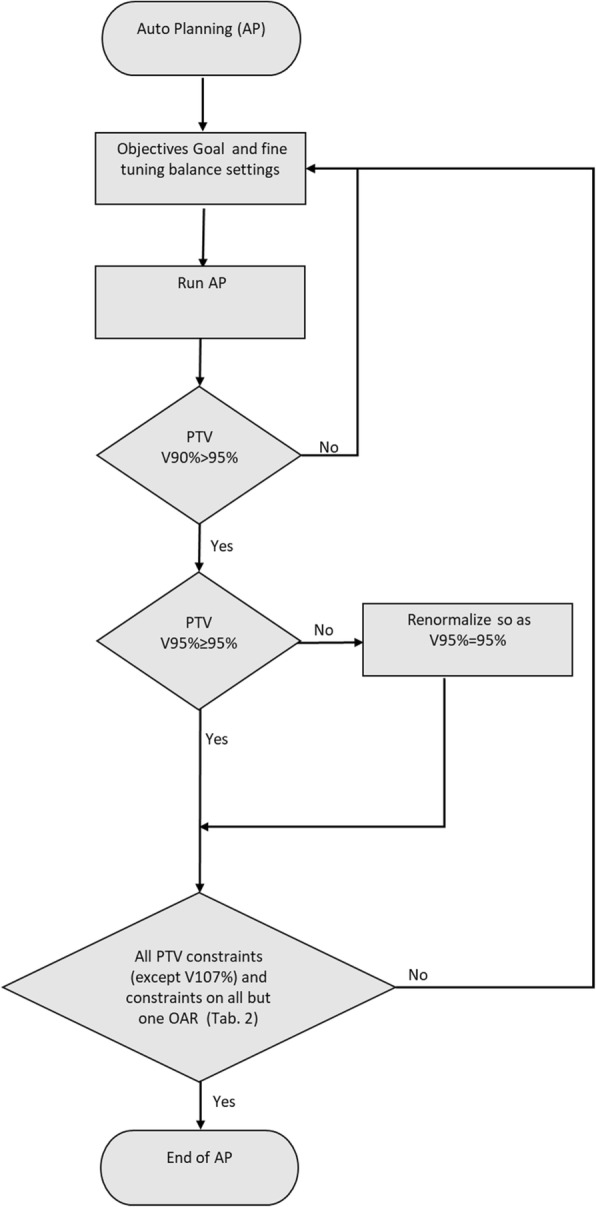
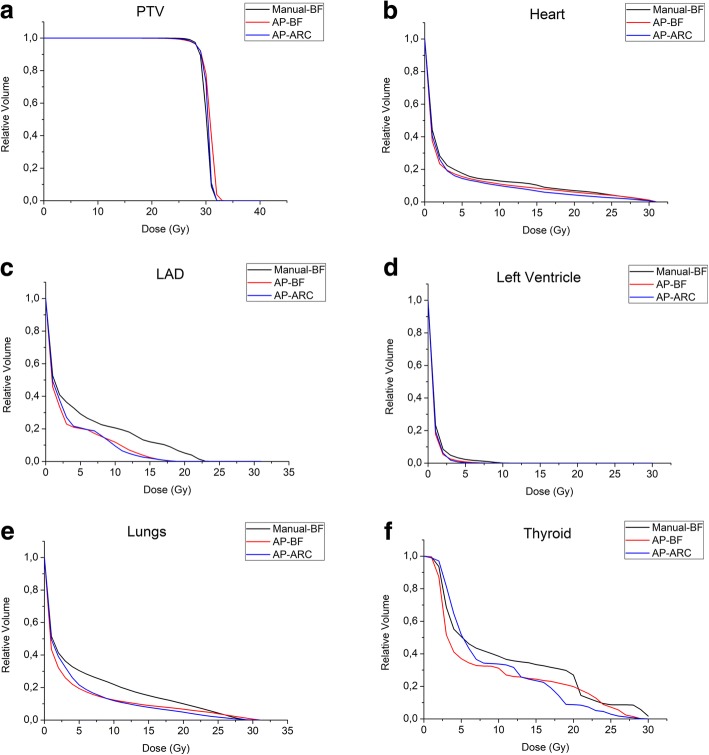
CT-scans of 10 female patients with SHL were considered. A "butterfly" (BF) volumetric modulated arc therapy was optimized using SmartArc module integrated in Pinnacle v. 9.10 using Collapsed Cone Convolution Superposition algorithm (30 Gy in 20 fractions). Human-driven (Manual-BF) and AP-BF optimization plans were generated. For AP, an optimization objective list of Planning Target Volume (PTV)/OAR clinical goals was first implemented, starting from a subset of 5 patients used for algorithm training. This list was then tested on the remaining 5 patients (validation set). In addition to the BF technique, the AP engine was applied to a 2 coplanar disjointed arc (AP-ARC) technique using the same objective list. For plan evaluation, dose-volume-histograms of PTVs and OARs were extracted; homogeneity and conformity indices (HI and CI), OARs dose-volume metrics and odds for different toxicity endpoints were computed. Non-parametric Friedman and Dunn tests were used to identify significant differences between groups.
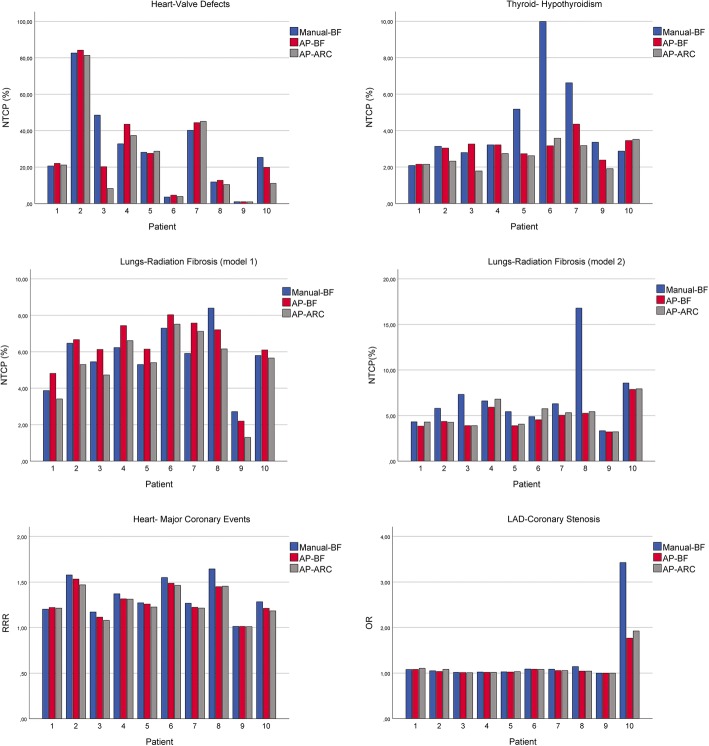
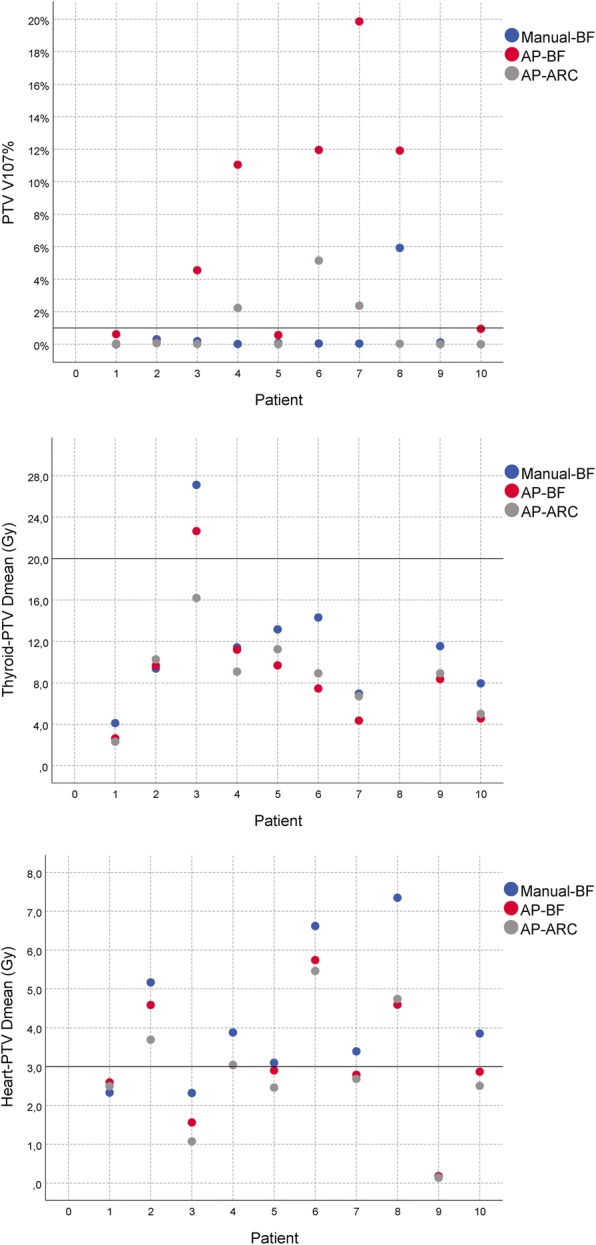
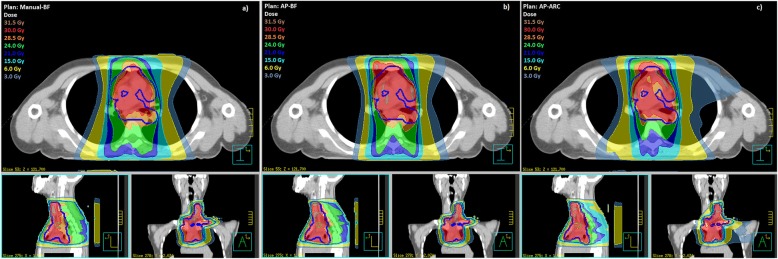
A single AP objective list for SHL was obtained. Compared to the manual plan, both AP-plans offer comparable CIs while AP-ARC also achieved comparable HIs. All plans fulfilled the clinical dose criteria set for OARs: both AP solutions performed at least as good as Manual-BF plan. In particular, AP-ARC outperformed AP-BF in terms of heart sparing involving a lower risk of coronary events and radiation-induced lung fibrosis. Hands-on planning time decreased by a factor of 10 using AP on average.
Despite the high interpatient PTV (size and position) variability, it was possible to set a standard SHL AP optimization list with a high level of generalizability. Using the implemented list, the AP module was able to limit OAR doses, producing clinically acceptable plans with stable quality without additional user input. Overall, the AP engine associated to the arc technique represents the best option for SHL.
霍奇金淋巴瘤(HL)放射治疗(RT)的技术进步通过高适形治疗有可能增加对危及器官(OARs)剂量分布的控制。然而,计划优化仍然是一项耗时的任务,并且具有很大的操作者依赖性变异性。本研究的目的是设计一个基于 Pinnacle 自动规划(AP)算法的全自动流水线,用于治疗女性膈上 HL(SHL)患者。
对 10 名女性 SHL 患者的 CT 扫描进行了研究。使用 Pinnacle v.9.10 中的 SmartArc 模块,结合 Collapsed Cone Convolution Superposition 算法(30Gy/20 次分割),对“蝴蝶”(BF)容积调制弧治疗进行了优化。生成了手动驱动(Manual-BF)和 AP-BF 优化方案。对于 AP,首先实施了一个包含计划靶区(PTV)/OAR 临床目标的优化目标列表,该列表从用于算法培训的 5 名患者子集开始。然后,将该列表应用于剩余的 5 名患者(验证集)。除了 BF 技术外,AP 引擎还应用于相同目标列表的 2 个共面不连续弧(AP-ARC)技术。为了评估计划,提取了 PTV 和 OAR 的剂量体积直方图;计算了均匀性和适形指数(HI 和 CI)、OAR 剂量体积指标以及不同毒性终点的概率。使用非参数 Friedman 和 Dunn 检验来确定组间的显著差异。
为 SHL 获得了一个单一的 AP 目标列表。与手动计划相比,两种 AP 计划都提供了可比的 CI,而 AP-ARC 也实现了可比的 HI。所有计划都满足了 OAR 设定的临床剂量标准:两种 AP 解决方案都至少与 Manual-BF 计划一样好。特别是,AP-ARC 在保护心脏方面优于 AP-BF,涉及冠状动脉事件和放射性肺纤维化的风险较低。平均而言,使用 AP 可将手动规划时间减少 10 倍。
尽管患者间 PTV(大小和位置)的变异性很大,但仍有可能设置一个具有高度通用性的标准 SHL AP 优化列表。使用实施的列表,AP 模块能够限制 OAR 剂量,生成具有稳定质量的临床可接受计划,无需额外的用户输入。总的来说,AP 引擎与弧形技术结合代表了 SHL 的最佳选择。