Infection Control Program and WHO Collaborating Center, Geneva University Hospitals and Faculty of Medicine, Geneva, Switzerland.
University Grenoble Alpes/CNRS, ThEMAS TIM-C, UMR 5525, Grenoble, France.
Intensive Care Med. 2018 Nov;44(11):1777-1786. doi: 10.1007/s00134-018-5227-4. Epub 2018 Oct 21.
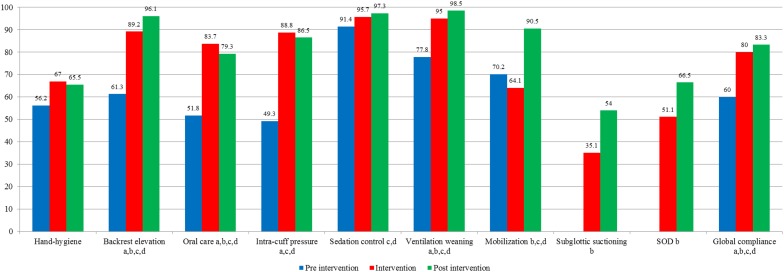
We describe the impact of a multifaceted program for decreasing ventilator-associated pneumonia (VAP) after implementing nine preventive measures, including selective oropharyngeal decontamination (SOD).
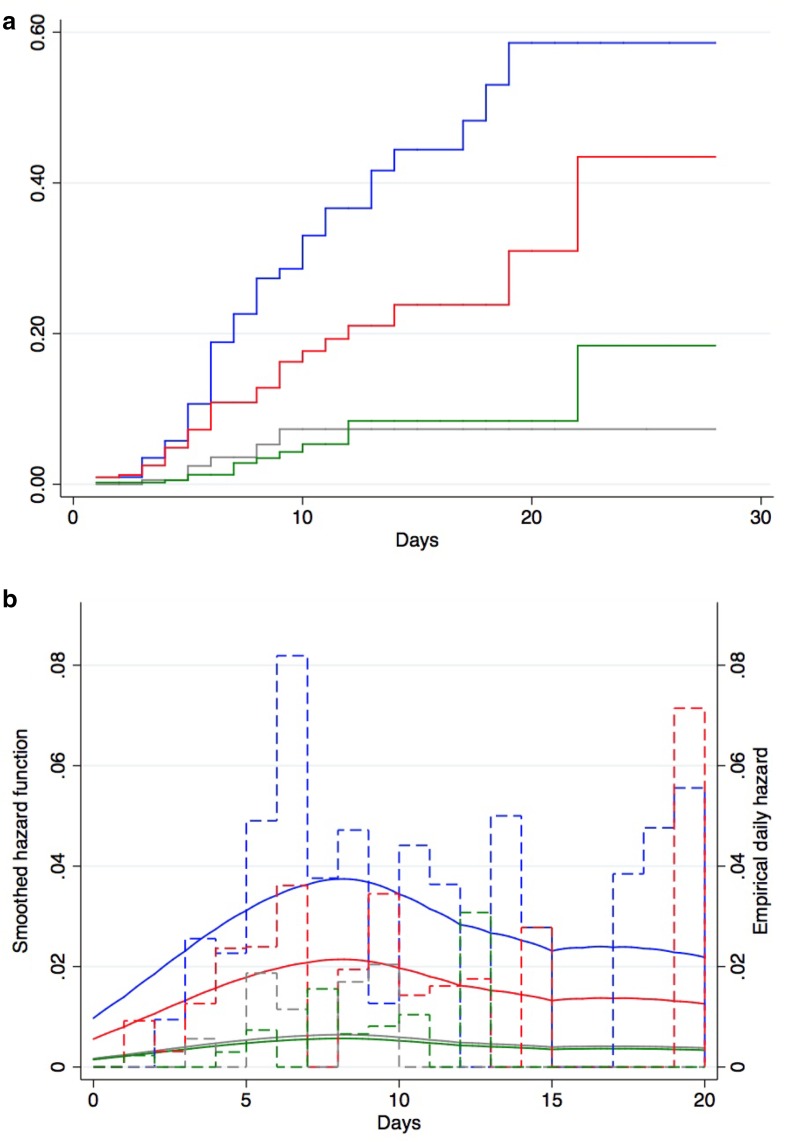
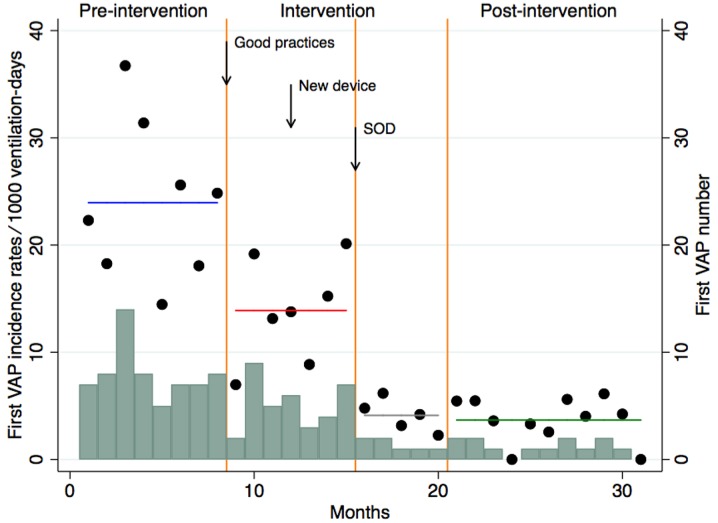
We compared VAP rates during an 8-month pre-intervention period, a 12-month intervention period, and an 11-month post-intervention period in a cohort of patients who received mechanical ventilation (MV) for > 48 h. The primary objective was to assess the effect on first VAP occurrence, using a Cox cause-specific proportional hazards model. Secondary objectives included the impact on emergence of antimicrobial resistance, antibiotic consumption, duration of MV, and ICU mortality.
Pre-intervention, intervention and post-intervention VAP rates were 24.0, 11.0 and 3.9 VAP episodes per 1000 ventilation-days, respectively. VAP rates decreased by 56% [hazard ratio (HR) 0.44, 95% CI 0.29-0.65; P < 0.001] in the intervention and by 85% (HR 0.15, 95% CI 0.08-0.27; P < 0.001) in the post-intervention periods. During the intervention period, VAP rates decreased by 42% (HR 0.58, 95% CI 0.38-0.87; P < 0.001) after implementation of eight preventive measures without SOD, and by 70% after adding SOD (HR 0.30, 95% CI 0.13-0.72; P < 0.001) compared to the pre-intervention period. The incidence density of intrinsically resistant bacteria (to colistin or tobramycin) did not increase. We documented a significant reduction of days of therapy per 1000 patient-days of broad-spectrum antibiotic used to treat lower respiratory tract infection (P < 0.028), median duration of MV (from 7.1 to 6.4 days; P < 0.003) and ICU mortality (from 16.2 to 13.5%; P < 0.049) for patients ventilated > 48 h between the pre- and post-intervention periods.
Our preventive program produced a sustained decrease in VAP incidence. SOD provides an additive value.
在实施九项预防措施后,包括选择性口腔去污(SOD),我们描述了降低呼吸机相关性肺炎(VAP)的多方面计划的影响。
我们比较了机械通气(MV)超过 48 小时的患者队列在干预前 8 个月、干预 12 个月和干预后 11 个月期间的 VAP 发生率。主要目的是使用 Cox 因果特定比例风险模型评估首次 VAP 发生的影响。次要目标包括对抗菌药物耐药性的出现、抗生素消耗、MV 持续时间和 ICU 死亡率的影响。
干预前、干预中和干预后 VAP 发生率分别为每 1000 通气日 24.0、11.0 和 3.9 例 VAP 。VAP 发生率分别下降了 56%(风险比[HR]0.44,95%CI0.29-0.65;P<0.001)和 85%(HR0.15,95%CI0.08-0.27;P<0.001)。在干预期间,在没有 SOD 的情况下实施八项预防措施后,VAP 发生率下降了 42%(HR0.58,95%CI0.38-0.87;P<0.001),在添加 SOD 后下降了 70%(HR0.30,95%CI0.13-0.72;P<0.001)与干预前相比。内在耐药菌(对粘菌素或妥布霉素)的发生率密度没有增加。我们记录到治疗每 1000 例患者-天广谱抗生素用于治疗下呼吸道感染的治疗天数显著减少(P<0.028),中位 MV 持续时间(从 7.1 天降至 6.4 天;P<0.003)和 ICU 死亡率(从 16.2%降至 13.5%;P<0.049)在干预前和干预后期间 MV 超过 48 小时的患者。
我们的预防计划持续降低了 VAP 的发病率。SOD 提供了附加价值。