Froehner Michael, Koch Rainer, Hübler Matthias, Heberling Ulrike, Novotny Vladimir, Zastrow Stefan, Hakenberg Oliver W, Wirth Manfred P
Department of Urology, University Hospital Carl Gustav Carus, Technische Universität Dresden, Fetscherstrasse 74, D-01307, Dresden, Germany.
Department of Medical Statistics and Biometry, University Hospital Carl Gustav Carus, Technische Universität Dresden, Fetscherstrasse 74, D-01307, Dresden, Germany.
BMC Urol. 2018 Oct 22;18(1):91. doi: 10.1186/s12894-018-0402-z.
Radical cystectomy bears a considerable perioperative mortality risk particularly in elderly patients. In this study, we searched for predictors of perioperative and long-term competing (non-bladder cancer) mortality in elderly patients selected for radical cystectomy.
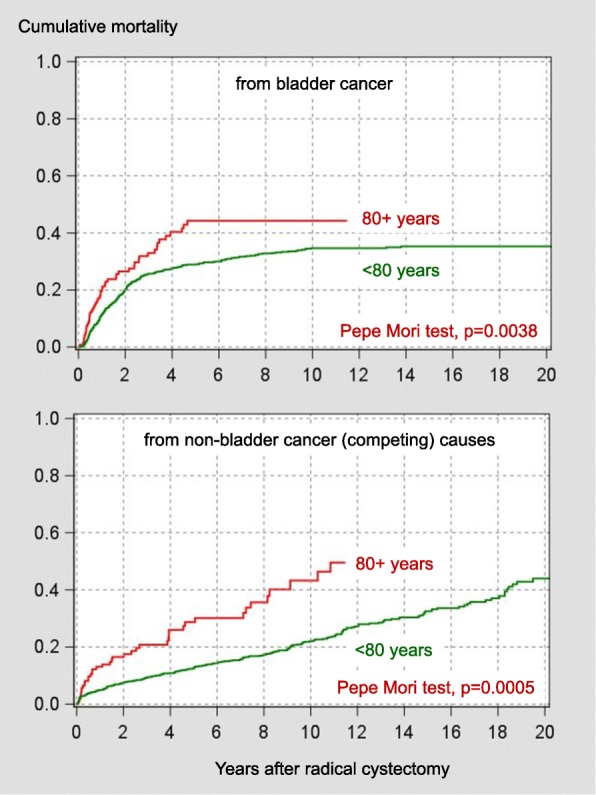
We stratified 1184 consecutive patients who underwent radical cystectomy for high risk superficial or muscle-invasive urothelial or undifferentiated carcinoma of bladder into two groups (age < 80 years versus 80 years or older). Multivariable and cox proportional hazards models were used for data analysis.
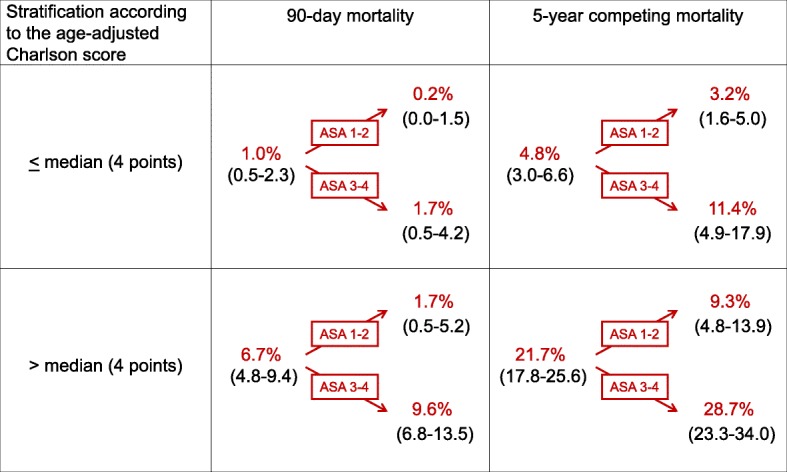
Whereas Charlson score and the American Society of Anesthesiologists (ASA) physical status classification (but not age) were independent predictors of 90-day mortality in younger patients, only age predicted 90-day mortality in patients aged 80 years or older (odds ratio per year 1.24, p = 0.0422). Unlike in their younger counterparts, neither age nor Charlson score or ASA classification were predictors of long-term competing mortality in patients aged 80 years or older (hazard ratios 1.07-1.10, p values 0.21-0.77).
This data suggest that extrapolations of perioperative mortality or long-term mortality risks of younger patients to octogenarians selected for radical cystectomy should be used with caution. Concerning 90-day mortality, chronological age provided prognostic information whereas comorbidity did not.
根治性膀胱切除术具有相当大的围手术期死亡风险,尤其是在老年患者中。在本研究中,我们寻找接受根治性膀胱切除术的老年患者围手术期和长期竞争性(非膀胱癌)死亡的预测因素。
我们将1184例因高危浅表性或肌层浸润性尿路上皮癌或膀胱未分化癌接受根治性膀胱切除术的连续患者分为两组(年龄<80岁与80岁及以上)。采用多变量和Cox比例风险模型进行数据分析。
在年轻患者中,Charlson评分和美国麻醉医师协会(ASA)身体状况分级(而非年龄)是90天死亡率的独立预测因素,而在80岁及以上患者中,只有年龄可预测90天死亡率(每年的比值比为1.24,p = 0.0422)。与年轻患者不同,年龄、Charlson评分或ASA分级均不是80岁及以上患者长期竞争性死亡的预测因素(风险比为1.07 - 1.10,p值为0.21 - 0.77)。
这些数据表明,将年轻患者的围手术期死亡率或长期死亡风险外推至接受根治性膀胱切除术的八旬老人时应谨慎使用。关于90天死亡率,实际年龄可提供预后信息,而合并症则不能。